Closure of the mesenteric defects in an ante-colic ante-gastric Roux-en-Y Gastric Bypass
May 2012
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS, and Daniel B. Jones, MD, MS, FACS
This month’s technique: Closure of the mesenteric defects in an ante-colic ante-gastric Roux-en-Y Gastric Bypass
This Month’s Featured Experts:
Alfons Pomp, MD, FACS, FRCSC
Leon C. Hirsch Professor, Vice Chairman, Department of Surgery Chief,Section of Laparoscopic and Bariatric Surgery, Weill Medical College of Cornell University New York Presbyterian Hospital, New York, New York
Co-Author
Amanda J. powers, MD
Minimal invasive Surgery Fellow, Weill Cornell Medical College/New York Presbyterian Hospital, New York, New York
Bariatric Times. 2012;9(5):10–11
Introduction
Internal hernias are a known complication of Roux-en-Y gastric bypass (RYGB) that are difficult to diagnose by history, physical exam, or radiographic imaging. The consequences of an unrecognized internal hernia leading to bowel ischemia can be devastating.
Closure of the mesenteric defects at the time of RYGB is generally accepted as standard of care although comparative studies are small and mostly retrospective. The surgeons at Weill Cornell Medical Center believe there is some reduction in complications secondary to internal hernia when we compared our present experience to results prior to the adoption of mesenteric closure. At Weill Cornell Medical Center, New York, New York, we routinely use an ante-gastric ante-colic Roux limb in the creation of the gastro-jejunostomy.
Procedure
Patient position. For RYGB, the patient is positioned supine with the legs split and well secured.
Trocar placement. Access to the abdominal cavity is obtained through the umbilicus and a 10mm reusable trocar is inserted. Under direct vision, a 5mm trocar is inserted in the sub-xyphoid position to the left of the falciform ligament. Two additional 5mm trocars are used in the right and left upper quadrants and a 12mm port is placed in the left mid-clavicular line halfway between the inferior costal margin and the level of the umbilicus.
Dissection of the gastric pouch and proximal anastomosis. The stomach pouch is created by identifying the gastroesophageal (GE) junction, then measuring a 5 to 6cm long pouch. After creation of the pouch, the transverse colon is retracted cephalad to expose the ligament of Treitz. Beginning at the ligament, the small bowel is measured to a length of approximately 100cm. While clearly maintaining the orientation of proximal versus distal, the small bowel is transected using an Endo GIA™ stapler (Covidien, Norwalk, Connecticut).
An orogastric tube armed with the anvil of an EEA™ OrVil™ 25 mm (Covidien) is passed by the anesthesiologist through the mouth into the proximal gastric pouch where a small opening is made. The orogastric tube is removed, leaving the anvil in place. The staples on the distal small bowel are removed and the left upper quadrant trocar site is enlarged to permit the introduction into the abdominal cavity of an EEA 25mm. Once in the abdominal cavity, the EEA is inserted into the opened distal small bowel for approximately 6cm where the spike perforates on the anti-mesenteric side under direct vision.
The stapler is joined to its complimentary anvil and a circular stapled anastomosis is created. The EEA is removed from the abdominal cavity in a sterile sheath. The opening in the small bowel is closed with a GIA stapler.
The distal anastomosis and closure of the entero-enterostomy defect. We measure caudad from the gastrojejunostomy approximately 150cm while orienting the bowel mesentery in a counterclockwise fashion. At this point, the proximal small bowel lies caudad to the proximal jejunum “stump” and this is easily anastomosed by creating two small openings on the antimesentric side of each small bowel, inserting and firing an Endo GIA stapler and closing the resulting unique opening with a running 2-0 resorbable suture. This technique of anastomosis brings together the mesentery of both of the small bowel limbs while at the same time exposing the mesenteric defect.
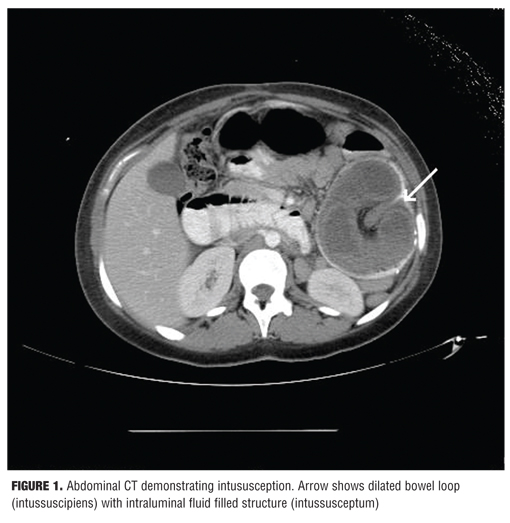
The mesenteries are closed from the apex of the distal small bowel to the base of the mesentery and back to the apex of the proximal small bowel in a purse string type fashion using a running 2-0 silk suture (Figure 1).
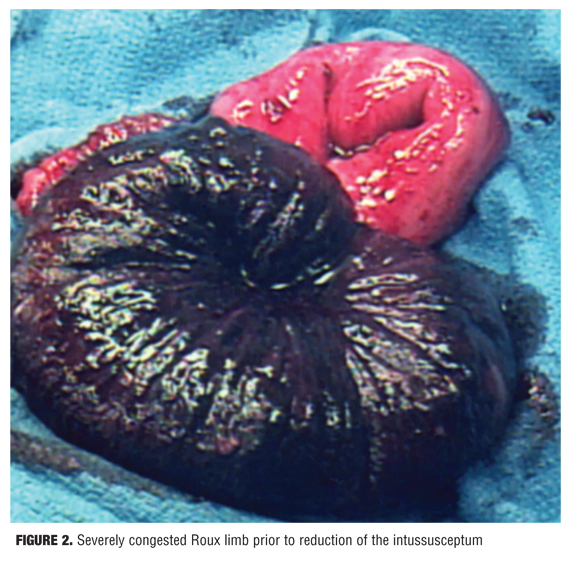
Closure of Peterson’s defect. In bariatric surgery, Petersen’s defect is defined as the space between the jejunal and transverse colonic mesentery after the creation of a gastrojejunostomy.
The adequate closure of this space is dependent on adequate exposure (Figure 2), which can be difficult with short thick mesentery and abundant intra-abdominal fat. The newly created alimentary limb must be deflected to the patient’s left side while the greater omentum lying to the patient’s right of the alimentary limb must be pushed cephalad above the transverse colon, and the colon itself must be maintained cephalad in order to splay its mesentery. This allows exposure of an apex of transverse colon mesentery and the inferior most portion of the small bowel alimentary limb mesentery which is where we start our closure.
We have elected to use running permanent suture (2-0 silk) cut to 28cm on a tapered needle. After an initial knot, several mesenteric “bites” are placed and then the adjacent mesenteries are closely approximated ending with the last suture through the transverse colon taenia to the mesenteric border of the ante-colic roux alimentary limb.
Suture choice. We elect to perform a running versus interrupted closure in order to facilitate a tight closure that will be less likely to develop into small defects with the expected future weight loss. Optimal suture choice in our experience is nonabsorbable braided suture, however, a nonabsorbable monofilament can also be used.
Pitfalls
Inadequate exposure may lead to partial closure of the defect which then creates smaller defects that may increase risk of incarceration/strangulation if herniation does occur. This can also occur with failure to include bowel wall as the last “bite” within the closure or failure to correctly identify the apex of the two mesenteries.
Stitches that are too superficial through mesenteric fat may pull through with tension and not provide adequate closure. Overly aggressive “bites” that stray from the mesenteric ridge may cause bleeding or kinking (shortening) of the mesentery that may lead to increased tension on the anastomosis.
Conclusion
The closure of the mesenteric defects remains a subject of controversy. The danger of partial closure, the added operating time, and the actual low incidence of bowel compromise due to internal hernia via these defects are all issues raised in the debate against routine closure.
The consequences of a missed symptomatic internal hernia, which is universally agreed to be a difficult diagnosis, can be very significant. We believe there are patient benefits if the mesenteric defect is properly closed.
Funding: There was no funding for the preparation of this manuscript.
Disclosures: Dr. Pomp reports no conflicts of interest relevant to the content of this article.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}