Endoscopic Revision of Roux-en-Y Gastric Bypass Stomal Dilation with a Suturing Device: Preliminary Results of a First Out-of-United-States Series
by Manoel Galvão Neto, MD; Leonardo Rodriguez, MD; Natan Zundel, MD; Juan Carlos Ayala, MD; Josemberg Campos, PhD; and Almino Ramos, MD
Drs. Galvão and Ramos are from Gastro Obeso Center, Sao Paulo, Brazil. Drs. Rodriguez and Ayala are from Clinica Indisa, Santiago, Chile. Dr. Zundel is from Florida International University, Miami, Florida, United States. Dr. Campos is from Federal University of Pernambuco, Brazil.
Bariatric Times. 2011;8(6):32–34Funding: Apollo Endosurgery, Inc. provided devices for the study presented in this article and cases were done under private insurance reimbursement.
Financial disclosure: Drs. Galvão, Ramos, and Zundel are international consultants for Apollo Endosurgery, Inc. Drs. Rodriguez and Ayala report no conflicts of interest relevant to the content of this article.
ABSTRACT
In this article, the authors describe the preliminary results of the first series outside of the United States conducted on Roux-en-Y gastric bypass endoscopic gastrojejunostomy stomal revision by means of an endoscopic suturing device, the OverStitch™. They examine the results of their retrospective series analysis evaluating the safety and short-term efficacy of the OverStitch endoscopic suturing system. Studies performed using the OverStitch and other endoscopic devices are discussed.
INTRODUCTION
Bariatric surgery has proven to be the most valuable treatment of morbid obesity by effectively lowering excess weight, controlling surrounding co-morbidities, and lowering mortality in patients with morbid obesity. The Roux-en-Y gastric bypass (RYGB) is among the most-performed bariatric procedures. Despite very good results, this procedure can fail in maintaining long-term weight loss with failure rates over 20 percent.[1]
Postoperative weight loss failures can be defined in many different ways. One of the most accepted parameters involves the patients’ ability to achieve and maintain 50 percent excess weight loss (EWL). If a patient who has undergone RYGB does not achieve 50 percent or more EWL, a surgical revision procedure may be required.[2,3] Surgical revisions after RYGB are, by nature, complex and associated with significant morbidity, and even questionable efficacy.[4,5]
Among possible causes of RYGB procedure failure is dilation of the gastro-jejunostomy (GJ), and/or gastric pouch enlargement.[6] The development of endoluminal therapies and devices for stoma revision can fulfill the need for a less-invasive approach that maintains some of the principles of surgical outlet revision while avoiding intra-abdominal surgery.
This article describes preliminary results of the first series outside the United States (OUS) of RYGB endoscopic GJ stomal revision by means of a novel endoscopic suturing device, the OverStitch™ Endoscopic Suturing System (Apollo Endosurgery, Inc. Austin, Texas).
AIM
The primary aim of this study was to evaluate safety of the OverStitch. The secondary aim was to examine short-term weight-loss efficacy of the OverStitch.
METHODS
This retrospective series analysis was performed with chart review approval from the Institutional Review Board (IRB) and with patients’ informed consent. The analysis focused on evaluating safety and short-term efficacy of the OverStitch endoscopic suturing device in patients with significant weight regain (i.e., 50≤ EWL) after RYGB who were at least two years post-RYGB and who had participated in multidisciplinary follow-up programs. Patients who met these criteria were then screened with endoscopy and xrays to determine if they had a gastro-jejunostomy over 2cm in diameter. Inability to undergo general anesthesia and/or an upper endoscopy excluded patients from this series.
Data on safety, intra- and postoperative complications, and weight-loss efficacy were recorded for up to 90 days. Also, data on pre- and postoperative stoma size, operative time, and the number of sutures applied at stomas were recorded. Stoma size was estimated before and after the procedure using endoscopic biopsy forceps of known open jaw-span distance. The length of the gastric pouch along the smaller curvature was estimated using endoscope markings.
The following were recorded: 1) patient weight before his or her primary RYGB, 2) patient-reported nadir (i.e., lowest) weight following primary RYGB, 3) patient weight before the endoscopic procedure, 4) regained weight, and 5) preprocedural pouch and stoma size. Postoperative weight loss or gains were recorded at 30, 60, and 90 days. Percentage of weight regain loss (WRL) was also recorded. After the procedure, a stepwise diet was initiated with clear liquids advancing to full solids at Week 4. Follow-up endoscopy was performed at three months postoperatively.
The Overstitch endoscopic suturing device is a cap-based suturing system that is mounted on a double-channel endoscope (GIF-2T160; Olympus Medical Systems Corporation, Tokyo, Japan). The curved needle arm mounts to the tip of the endoscope. The anchor is passed through the primary channel and acts like a needle that is passed back and forth between the needle arm and the anchor exchange (Figure 1). When the handle (Figure 2) is closed, the tissue anchor is advanced through the tissue into the anchor exchange (Figure 1). When suturing is complete the tissue anchor is released. The proximal end of the suture is then secured by advancing a Cinch device (Figure 3), which is used to securely lock and cut suture. The procedure is done under general anesthesia with the patient intubated. An esophageal overtube (US Endoscopy, Mentor, Ohio) is positioned to grant safe access (Figure 4). The pouch and stoma size were measured and the operating surgeon applied sutures at the level of the GJ, moving from the lesser to the greater curvature (Figure 5 and Figure 6), measuring its size at the end (Figure 7).
RESULTS
Eight patients (7 in Clinica Indisa, Chile, and 1 in Fundacion Santa Fe, Colombia) were submitted to the procedure providing safety and intra-operative efficacy data. At the time this article was sent for publication, four patients had completed 90 days follow up and provided postoperative weight loss and complication data. Patients included seven women and one man aged 28 to 58 years (Mean [M]=40.5 years), pre-RYGB BMI of 38 to 44kg/m2 (M=40.4kg/m2), pre-RYGB weight from 97 to 138kg (M=111kg), weight loss nadir (minimum weight loss from 87 to 60kg (M=67.8kg) and weight regain of 9 to 33kg (M=22kg). Pre-procedure pouch size varied from 2 to 6cm (M=3cm) and pre-procedure stoma size varied from 20 to 40 mm (M=25mm).
All patients had the procedure under general anesthesia and intubatation with the use of an esophageal overtube to assure safe access. Procedure time ranged from 20 to 60 minutes (M=38 minutes). All but one patient had three stiches applied from the lesser to the greater curvature of GJ, reducing the stoma size to a 10mm diameter. In one patient, the stoma size was reduced to 15mm. No intra-operative complications were noted.
Postoperative weight loss up to 90 days in four patients varied from 6 to 8kg with a mean percent RWL of 28 percent. No postoperative complications were recorded.
DISCUSSION
As the number of bariatric surgeries, including RYGB, increases into the hundreds of thousands annually, it is natural that weight loss failure rates will also increase proportionally. The reported RYGB failure rate varies widely, from less than 10 percent to 50 percent, depending on the assessment parameters.[1–3] Surgical societies, such as the Brazilian Society of Metabolic and Bariatric Surgery (SBCBM), tend to use parameters like 50 percent EWL to identify success. Clinical societies tend to use 20 to 30 percent EWL or resolution of comorbidities.[13]
Patients who have regained weight to a condition of morbid obesity while under multidisciplinary surveillance should consider revision surgery. A revision on an RYGB procedure can be done on its restrictive component (the gastric pouch and the GJ) or at its malabsorptive/metabolic component (bowel limb lengths). Surgical revisions of the RYGB are always a matter of concern due to higher rates of complications and mortality when compared with primary series.[4,5]
Revision of limbs has proven effective despite its implications for patients’ nutritional status.[1] On the other hand, pouch and stoma size have always been a matter of discussion in regards to how effectively they contribute to weight loss on RYGB. Recently, an article by Abu Dayyeh BK, Lautz DB, and Thompson CC from Massachusetts General Hospital, Boston, has shown that GJ size matters. The authors evaluated 165 patients with 59 percent of significant weight regain of 30 percent (±22%) where the GJ stoma diameter was significantly associated with weight regain after RYGB surgery in a univariate analysis (beta= 0.31, P< 0.0001) also serving as prediction rule for weight regain after RYGB with a positive predictive value of 75 percent.[6]
At the same time, endoluminal endoscopic procedures and devices are rapidly advancing to provide safe revision in RYGB on its restrictive components, although the efficacy of such procedures and devices needs further consideration. Endoscopic revisions on gastric pouch and GJ can be as simple as endoscopic injections of sclerosant agents like sodium morrhuate[7] and even tissue expanders like Polimetilmetacrilate (PMMA).[8] Revisions may also take advantage of sophisticated devices that can apply endoscopic sutures and anchors.[9–11] Thompson et al[10] reported that six of the eight patients with GJ over 2cm who underwent endoscopic anastomotic reduction with the Bard® EndoCinch™ Suturing System (C.R. Bard Inc., Murray Hill, New Jersey) resulting in a mean 10kg weight loss and 23.4 percent EWL at four months.[10] Brengman et al[12] reported eight patients with RYGB pouches revised with the Incisionless Operating Platform™ (USGI Medical, San Clemente, California) resulting in a mean 12.1kg weight loss and 33 percent EWL at 12 months.
This present OUS series demonstrates the safety of a novel endoscopic suturing device to revise GJ of failed RYGB and provides limited data on short-term efficacy. Using the same device, Jirapinyo et al,14 in a Digestive Disease Week 2011 congress presentation (the authors acknowledge thanks for the data provided by Dr. Christopher C. Thompson) reported its use on 22 patients’ pouches and GJs, adding the use of tissue ablation with argon plasma coagulation (APC) at GJ level. Sixteen out of 22 patients (72.7%) were women with average time from RYGB of 6±2 years, stomal diameter of 25.5±4.3mm (measured with an endoscopic measure stick ) and pouch length of 5.3±2.0cm. Mean procedure time was 28.6±21.6 minutes with a mean of three stitches. They achieved technical success in all patients with a 78-percent reduction in stoma diameter to 5.6+1.9 mm. There was one esophageal abrasion due to the overtube and one instance of bleeding at a suture spot. Four patients complained of nausea/vomiting and one patient required dilation.
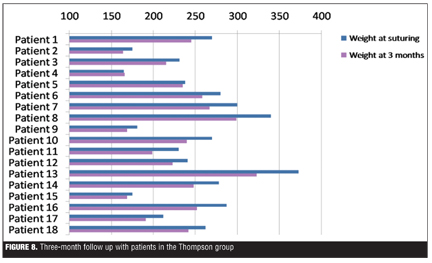
At three-month follow-up, patients in the Thompson group achieved 60.39 percent WRL and 21.45 percent EWL (Figure 8). It was noted that two patients in the Thompson group did not lose significant weight. These two patients were unique in that they had outlets sutured to 3–4mm and experienced postoperative emesis that potentially led to torn sutures.
In comparison to the current series, the Thompson group demonstrated improved weight loss. This can be explained by the more aggressive pursuit of GJ and pouch reduction by Dr. Thompson’s group (stomal diameter less than 10mm) and the use of APC in combination with sutures to provide restriction, whereas the authors of this series targeted a final GJ diameter greater than 10mm and used the suturing device exclusively without APC. In future studies, a balance of techniques should provide more definitive results.
CONCLUSION
In our experience, we found the OverStitch endoscopic device provides a technically feasible and safe means to reduce GJ stoma diameter. This device shows promise in the endoscopic treatment of weight regain after RYGB. However, longer-term results and larger series are needed to fully assess efficacy. This technology may also have additional application in the endoscopic repair of other bariatric surgery complications.
References
1. Christou N, Look D, MacLean L. Weight gain after short- and long-limb gastric bypass in patients followed for longer than 10 years. Ann Surg. 2006;244:734–740
2. Nesset EM, Kendrick ML, Houghton SG, et al. A two-decade spectrum of revisional bariatric surgery at a tertiary referral center. Surg Obes Relat Dis. 2007;3(1):25–30
3. Magro DO, Gelonese B, Delfini R, et al. Long-term weight regain after gastric bypass: a 5-year prospective study. Obes Surg. 2008;18(6):648–651
4. Schwartz R, Strodel W, Simpson W, Griffen W. Gastric bypass revision: lessons learned from 920 cases. Surgery. 1988;104:806–12
5. Gagner M, Gentileschi P, De Csepel J, et al. Laparoscopic reoperative bariatric surgery: Experience from 27 consecutive patients. Obes Surg. 2002;12:254–260
6. Abu Dayyeh BK, Lautz DB, Thompson CC. Gastrojejunal stoma diameter predicts weight regain after Roux-en-Y gastric bypass. Clin Gastroenterol Hepatol. 2011;9(3):228–233. Epub 2010 Nov 17
7. Catalano M, Rudic G, Anderson A, Chua Y. Weight gain after bariatric surgery as a result of a large gastric stoma: endotherapy with sodium morrhuate may prevent the need for surgical revision. Gastrointest Endosc. 2007;66(2):240–245.
8. Campos JM, Galvao Neto MP, Moura EGH. Endoscopia em cirurgia da obesidade. First Edition. São Paulo: Santos; 2008.
9. Schweitzer M. Endoscopic intraluminal suture plication of the gastric pouch and stoma in postoperative Roux-en-Y gastric bypass patients. J Laparoendosc Adv Surg Tech A. 2004;14:223–226.
10. Thompson C, Slattery J, Bundga M, Lautz D. Peroral endoscopic reduction of dilated gastrojejunal anastomosis after Roux-en-Y gastric bypass: a possible new option for patients with weight regain. Surg Endosc. 2006;20:1744–1748.
11. Herron D, Birkeet D, Bessler M, Swanstrom L. Gastric bypass pouch and stoma reduction using a transoral endoscopic anchor placement system: a feasibility study. Surg Endosc. 2007;21:S333.
12. Brengman ML, Schroder Gregory. 12-Month outcomes after revision of post Roux-en-Y bypass stomal and pouch dilation with an endoscopic tissue anchoring system: a prospective case series report. Bariatric Times. 2010;7(6):14–17
13. Brethauer SA, Pryor AD, Chand B, et al. Endoluminal procedures for bariatric patients: expectations among bariatric surgeons. Surg Obes Relat Dis. 2009;5(2):231–236.
14. Jirapinyo P, Dayyeh BKA, Slattery J, et al. Endoscopic repair of dilated gastrojejunal anastomoses using a novel endoscopic suturing device. Presented at: The annual meeting of The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES); March 30–April 2, 2011; San Antonio, Texas.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}