How to Perform an Antiobstruction Stitch
This Month’s Featured Expert
Robert E. Brolin, MD, FACS
Dr. Brolin is Adjunct Professor, University of Pittsburgh, Pittsburgh, Pennsylvania, and Director, Bariatric Surgery
University Medical Center at Princeton, New Jersey.
Bariatric Times. 2011;8(9):8–9
Introduction
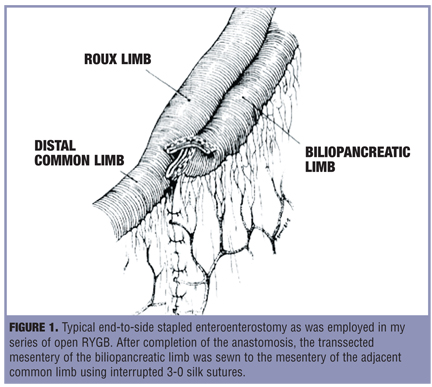
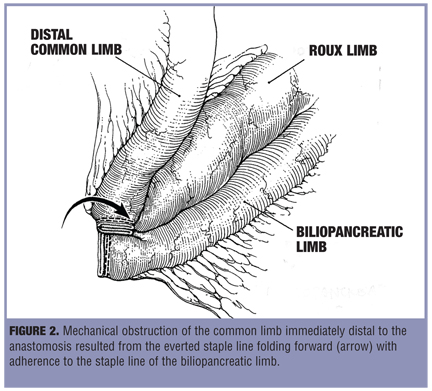
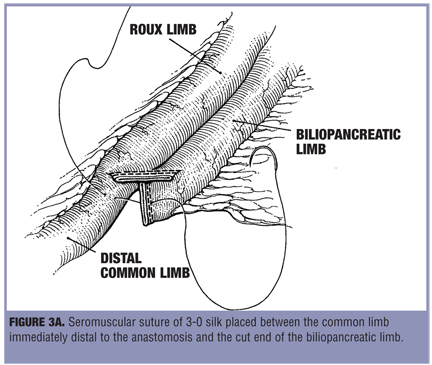
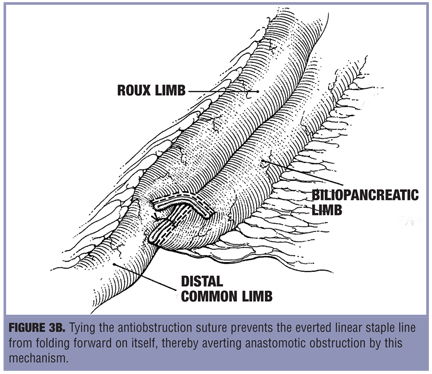
In 1994, I described a simple method of preventing small bowl obstruction that resulted from kinking of the bowel at the jejunojejunostomy following Roux-en-Y gastric bypass (RYGB).[1] In fact, three of my first 38 patients who had RYGB developed this type of obstruction. Two of these three patients required surgery. In each case, obstruction was caused by the everted stapled closure of the enteroenterostomy folding forward on itself and blocking antegrade flow beyond this point (Figure 1 and Figure 2). At laparotomy, the adherent staple lines were separated by sharp dissection, which relieved the obstruction. In order to prevent subsequent obstruction via the same mechanism, the common limb immediately distal to the anastomosis was sutured to the stapled end of the biliopancreatic (BP) limb. This “antiobstruction” stitch fixed the position of the everted staple lines thus preventing refolding of the bowel (Figure 3a and Figure 3b). Following these two operations that I performed in 1984, I have routinely used the antiobstruction stitch in all of my primary RYGBs. There have been no cases of obstruction at the jejunojejunostomy in 1,392 consecutive open RYGBs performed during the past 26 years.
Performing the Antiobstruction Stitch after Open RYGB versus Laparoscopic RYGB
During the past nine years, my facility saw five cases of obstruction at the jejunojejunostomy following 873 consecutive laparoscopic RYGBs. All five patients required surgery. Four of these five cases were recognized during the first three years of our laparoscopic experience, including two kinks and two strictures. The two kinks were clearly technical problems that were caused by narrowing of the lumen associated with the stapled closure of the enterotomy. In each case, misalignment of the closure was associated with an unusually small caliber lumen. All three of the strictures presented as obstruction of the BP limb. One patient was readmitted with BP limb obstruction on the Postoperative Day 4. The remaining two strictures were recognized several months postoperatively. These two patients had more insidious symptoms and were eventually diagnosed by abdominal computed tomography (CT) scan. The etiology of the three strictures was unclear at the time of reoperation; however, in each case the antiobstruction sutures appeared to be intact. There were no subsequent complications in any of these patients.
The incidence of obstruction at the jejunojejunostomy appears to be higher after laparoscopic RYGB in comparison with the open technique.[2,3] Although there are no controlled studies that compare specific techniques of performing the jejunojejunostomy, a number of laparoscopic bariatric surgeons have abandoned stapled closure of the enteroenterostomy in favor of some method of sutured closure.[4]
My placement of the antiobstruction stitch in laparoscopic cases is similar but not identical to its placement during open RYGB. This difference is primarily related to the position of the Roux limb relative to the colon. I have used a retrocolic, antegastric technique in all of the open cases. Conversely, all of the laparoscopic RYGBs were performed using an antecolic, antegastric approach. The difference in orientation of the Roux limb between the two approaches has a direct bearing on closure of the mesenteric defects. In laparoscopic cases, we frequently place more than one antiobstruction stitch. The antiobstruction stitch closest to the mesentery is used as the apex of the mesenteric closure, which is performed with a continuous 2-0 silk suture that opposes the cut edge of the BP limb and the mesentery of the Roux limb. In open RYGB, I close the mesenteric defects with interrupted 3-0 silk sutures as shown in Figure 1.
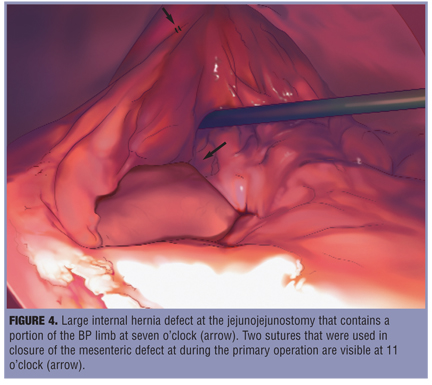
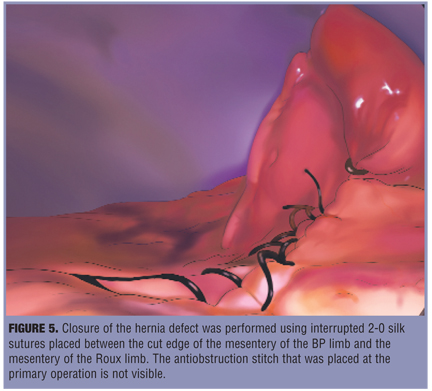
My initial technique of mesenteric closure in laparoscopic RYGB did not completely close the so called jejunojejunostomy defect. About two years after my first laparoscopic RYGB, we began to see patients with acute small bowel obstruction (SBO) from mesenteric internal hernias. We also recognized that many patients who developed acute SBO had lesser episodes of abdominal pain prior to developing complete obstruction.[4] Figure 4 shows a large hernia defect in a patient with intermittent abdominal pain who was admitted for elective laparoscopy. Figure 5 shows the completed repair. We routinely recommend elective laparoscopy in patients who have intermittent bouts of nausea, abdominal pain, and distention following laparoscopic RYGB.[5]
Conclusion
The antiobstruction stitch has been effective in aligning the stapled jejunojejunostomy so that patency is maintained and kinking is prevented. This stitch is easily incorporated in closure of the mesenteric defect in antecolic, antegastric RYGB.
References
1. Brolin RE. The anti-obstruction stitch in stapled Roux-en-Y enteroenterostomy. Am J Surg. 1995;169:355–357.
2. Podnos YD, Jimenez JC, Wilson SF, et al. Complications after laparoscopic gastric bypass: a review of 3464 cases. Arch Surg. 2003;138:957–961.
3. Capella RF, Iannace VA, Capella JF. Bowel obstruction after open and laparoscopic gastric bypass surgery for morbid obesity. J Am Coll Surg. 2006; 203: 328–335.
4. Brolin RE et al. Personal communication. 2004.
5. Gandhi AD, Patel RA, Brolin RE. Elective laparoscopy for herald symptoms of mesenteric/internal hernia after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2009; 5:144–149.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
cant see the figures mentioned in the article
Corrected. thanks for letting us know.