
Keeping the Bariatric Patient’s Skin Intact
This CE activity is expired.
by ‘Lissa Clark, RN, BSN, MSN, CNE, and Joyce M. Black, PhD, RN, CWCN, FAAN
Dr. Black is Associate Professor of Nursing, Department of Adult Health and Illness, University of Nebraska Medical Center, Omaha, Nebraska. Ms. Clark is Instructor of Nursing, Department of Adult Health and Illness, University of Nebraska Medical Center College of Nursing, Omaha, Nebraska
Financial disclosure: Dr. Black is a consultant for Coloplast Corporation and KCI. Ms. Clark reports no conflicts of interest relevant to the content of this article.
Funding: This CE-accredited article was supported by an educational grant from KCI.
Bariatric Times. 2011;8(5):20–23
Abstract
The authors review skin integrity issues specific to the bariatric patient population. Turning and repositions techniques are reviewed as well as prevention and management techniques. A case example is provided for illustrative purposes.
Introduction
Keeping the skin of patients intact has always been a goal of healthcare providers for many reasons; including pain, risk of infection, increased cost, and increased length of stay. In 2008, a financial reason was added to the list when the Centers for Medicare and Medicaid Services (CMS) determined that hospitals would not receive payment for specified hospital-acquired conditions, including pressure ulcers.[1] This provision makes it even more important for healthcare providers to take preventive actions to preserve skin integrity.
This article will examine some specific skin integrity issues affecting bariatric patients and discuss actions healthcare providers can take to prevent and/or treat them.
Case Example
A nurse working on an acute care floor had overheard Mrs. Porter, a patient on the unit, speaking to an attorney on the phone about the pain she was having with her pressure ulcers A flash was seen coming from the room and then it was noted that Mrs. P’s sister was taking a photograph of Mrs. P’s buttocks with her cell phone.
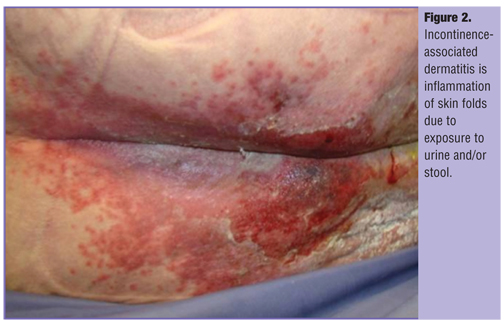
Mrs. P was a 62-year-old woman who was admitted to the hospital a week prior to this incident with shortness of breath. She was diagnosed with pneumonia. Because of her dyspnea and hypoxia, she was placed on bi-level positive air pressure (Bi-PAP) for decreased oxygen saturations. She appeared to have impending respiratory distress, so she was transferred quickly from the emergency room to the critical care unit and was placed on the standard hospital bed. Mrs. P was 64” tall and had a verified weight of 403 pounds, with a body mass index (BMI) of 69kg/m2. Her abdominal girth was 42 inches. Because of her severe dyspnea, her preferred position in bed was with the head of the bed elevated to 45 degrees in the Fowler’s position. She had a past medical history that included type 2 diabetes mellitus (T2DM) with prescribed oral medications, gastroesophageal reflux disease (GERD), and venous ulcers of the lower extremities. During the admission assessment, intertriginous dermatitis (ITD) was found under both breasts and the abdominal panniculus. ITD is inflammation of opposing skin surfaces in skin folds caused by moisture and exacerbated by friction and heat (Figure 1). A pillowcase was found beneath each breast and a bath towel folded in the panniculus. Her undergarments were wet with urine and incontinence-associated dermatitis (IAD), inflammation of the perineal skin related to chronic exposure to urine and/or liquid stool, was found throughout her perineal area and up the buttocks (Figure 2).
During the intervening days, her oxygen saturations were volatile. She would often remove the Bi-PAP mask due to feelings of suffocation. She developed an ulcer on the bridge of her nose under her Bi-PAP mask. She was difficult to move in bed and out of bed. She would flail her arms and become anxious with any movement. During one attempt to move her to the bedside chair, she slipped down to the floor and the skin on both forearms tore. Two days post-admission, the staff noticed a deep purple area across her buttocks. This area was identified by a nurse as deep tissue injury (DTI). DTI is a type of pressure ulcer that develops when pressure is high on any part of the body without relief. DTI presents as purple, intact tissue 48 hours after the unrelieved pressure is exerted. This type of pressure ulcer develops quickly and always evolves into a full-thickness (i.e., Stage 3 or 4) ulcer.
Pressure ulcers
Pressure ulcers are the result of pressure depriving tissue of blood; therefore, turning patients to relieve pressure is essential. A supine patient’s body must be turned in the bed to a full 40-degree lateral angle in order to lift the sacrum, the large, triangular bone at the base of the spine and at the upper and back part of the pelvic cavity, from the bed. It is not adequate to simply shift the “shelves” of adipose tissue; the patient’s frame or skeleton must be turned. In Mrs. P’s case, the standard hospital bed, which is 35 inches wide, prohibited her from being turned effectively. In addition, the standard mattress was quickly compressed by her body weight to the point that she was resting on the bed frame. Intense pressures that developed in this situation, combined with the inability to move the patient lead to the development of DTI, which would later evolve into full-thickness pressure ulcers if not treated effectively.
It is crucial that bariatric patients be placed in appropriate beds from the time of admission. Once a bariatric patient is placed into a standard hospital bed, it is cumbersome and difficult to transfer them into another bed. In order to ensure quick availability and delivery, it is recommended that a number of these beds be kept in storage at the hospital as opposed to off-site storage. In addition, a policy should be in place for communication between the emergency department (ED) and the admissions areas to notify the nursing unit when a bariatric patient is going to be hospitalized in order for the bariatric bed to be in place when the patient arrives.
Turning and Repositioning
Turning and repositioning are crucial for all patients confined to bed. Fatigue, dyspnea, and the width of the bed limited Mrs. P’s ability to turn and reposition herself adequately. The standard of care with customary equipment requires a dependent patient be turned every two hours. Turning patients with obesity safely and adequately requires adequate staff and equipment and should never be done alone. Attempting to lift, turn, or reposition a patient alone can cause injury to both the patient and the caregiver. It is suggested that staff collaborate by coordinating planned turning times in advance. An effort must be made to develop a program that helps staff, the patient, and the patient’s skin. In addition, care must be taken to obtain buy-in from staff and patients to facilitate compliance, cooperation, and improve outcomes.
The deep tissue injury that developed in Mrs. P would likely require weeks of treatment. Until recently, little evidence was available for the treatment of DTI except to turn the patient off of the involved area and to provide appropriate wound care. Today, there is some early evidence for early resolution without full thickness tissue loss with ultrasonic MIST® therapy (Celleration, Eden Prairie, Minnesota).[3] MIST therapy is thought to decrease inflammatory cytokines in the tissue of the wound. It is unacceptable to let DTI occur before a turning schedule is initiated.
Equipment. In addition to specialty beds made for bariatric patients, important equipment includes a trapeze, unless contraindicated for medical reasons, and an over-bed lift system adequate for the patient’s weight. Many equipment-associated injuries that occur are the result of user error and can be decreased with staff education and in-services.
Over-bed lift systems utilize fabric slings underneath patients during lifts. These slings must be removed after each lift. The caregiver should consider the fabric of the sling; if made from canvas it has no pressure redistribution properties. If left under the patient after the lift, the desired effect may be negated.
Prevention and Management of Skin Injuries
Shear. Shear is the force applied to tissue when pulled in two directions. A good example of this is the painful ripping sensation when arising from a vinyl chair when wearing shorts. In the case of Mrs. P, the force of gravity was pulling on her torso while the skin was held onto the bed. For patients at risk for pressure ulcer and shear, the head of the bed should never be raised above 30 degrees unless it is indicated medically. Pressure ulcer risk peaks when the head of the bed is raised to 45 degrees and pressure is not relieved. In this position, gravity pulls the patient’s torso down, sliding it against the bed. It is also important to consider the microclimate, the heat and moisture at the skin/bed interface. Microclimate is considered the newest facet in pressure ulcer etiology. The skin-surface interface becomes hot and humid very quickly in patients with extreme obesity because they must perspire to maintain their body temperature. In addition, the standard mattress cover does not “breathe,” so heat and moisture build up in this space between the skin and mattress. This wet, warm skin does not glide on the mattress cover and linen, which produces an increased risk of shear injury and pressure ulcers.
The presence of moisture in the microclimate makes the skin less likely to slide freely, which enhances shear. Pretreating the sacrum with a silicone dressing has been shown to reduce shear and prevent pressure ulcers when the head of the bed must be elevated, as in Mrs. P’s case.[4]
Managing the microclimate. The microclimate is best managed with a support surface that both cools and dries the patient’s skin at the interface between the bed and the body of the patient. Low air-loss mattresses have traditionally been used for this purpose. However, they are only effective for microclimate management if the patient is turned regularly, because the patient’s body occludes the holes in the mattress, thereby negating the benefit. Use of proper bed linens is also important. Microclimate can also be managed by turning, ambulation, and use of specialized support surfaces designed to cool and dry the skin at the interface.[5]
Skin tears. A skin tear is a flap-like separation of the epidermis from the underlying dermis and is most often associated with shear.[6] Bariatric patients are at an increased risk for skin tears because of the additional effort necessary for transfer and repositioning. This type of injury can be reduced with an education program on safe transfer and positioning techniques for caregivers. Patients should be assessed for additional factors that may put them at risk, such as corticosteroid use. Care for skin tears involves use of nonadherent dressings with additional absorptive dressings, as appropriate.[7]
Incontinence-associated dermatitis (IAD). The prevention and care of IAD are similar. Both prevention and care of this condition include a three-pronged, consistent skin care regimen of prompt removal of urine and stool, cleansing of the area, application of a moisturizer, and use of a skin protectant. Absorptive products should be used appropriately and changed often. Diversion devices, such as indwelling urinary catheters and fecal drainage systems, have been shown to prevent IAD, but have inherent risks that must be considered,[8] such as urinary tract infection and tissue injury. Care should also be taken to differentiate between IAD and Stage 1 and 2 pressure ulcers. The most pertinent assessment is the location. IAD tends to occur in areas where urine accumulates. Pressure ulcers usually develop over bony prominences or under areas exposed to pressure from medical devices.[8]
Intertriginous dermatitis (ITD). Prevention of ITD includes reduction of friction between the body folds, reducing heat and moisture in the skin folds, and maintaining proper hygiene. Friction can be reduced by using a patting motion when washing and drying and using soft baby washcloths or disposable cleansing cloths. Skin folds must be visualized to the base. This may require assistance when lifting folds of bariatric patients. Candidiasis, an infection caused by a yeast-like fungus called candida (Candida albicans), has long been thought to be the predominant infecting organism in skin fold dermatitis. However, a study of the cultures of skin folds showed that only 31 percent of present organisms comprised candida. In this study, cultures of skin folds grew many of the bowel organisms, including Proteus mirabilis, Enterococcus faecalis, Vancomycin-resistant enterococcus, and Escherichia coli.[9] When candida is present, a light dusting of antifungal powder can be used.
However, silver-impregnated wicking fabric has been shown to eradicate bacterial pathogens.10 In a recent consensus document, Black et al[8] determined the commonly used interventions, such as placing linens and/or talc in the body folds, were ineffective and may actually exacerbate skin damage. (Figure 3)
Mrs. P—Rewind
On admission for pneumonia, Mrs. P was placed on a bariatric bed with a microclimate-management surface. Her sacrum was pretreated with a silicone dressing to reduce shear. Small strips of hydrocolloid dressing were placed on the bridge of her nose to prevent skin breakdown from her Bi-PAP. A silver-impregnated textile was placed in all skin folds, and an indwelling urinary catheter was placed to divert urine from her perineum. A consistent skin care routine was initiated, which included gentle cleansing, moisturizing, and application of a skin protectant. Mrs. P was consistently repositioned; and she got out of bed with assistance using an overbed lift. The fabric sling was removed from under her between lifts. A week after admission, Mrs. P had no new areas of skin breakdown and both her IAD and ITD showed signs of healing. Best of all, the malpractice attorney had to find a new case.
References
1. Black J, Edsberg L, Baharestani, M, et al. Pressure ulcers: avoidable or unavoidable? Results of the National Pressure Ulcer Advisory Panel consensus conference. Ostomy Wound Manage. 2010;57(2):24–37.
2. Leen M. Establishing a comprehensive bariatric protocol. Nurs Manage. 2010;41(5):47–50.
3. Honaker J, Forston M, Davis E, et al. Effect of noncontact low-frequency ultrasound treatment on suspected deep tissue injury healing. Presented at: The 12th Biennial National Pressure Ulcer Advisory Panel (NPUAP) Consensus Conference; 2011: Las Vegas, NV.
4. Brindle C. Outliers to the Braden Scale: identifying high risk ICU patients and the results of prophylactic dressing use. World Council of Enterostomal Therapists. 2009;30 (1):11–18.
5. Clark M, Black J. International review. Pressure ulcer prevention: pressure, shear, friction and microclimate in context. A consensus document. Wounds Int. 2010:2–10;19–24. www.wounds
international.com/pdf/content_8925.pdf. Accessed May 3, 2011.
6. Le Blanc K, Barnoski S. Prevention and management of skin tears. Adv Skin Wound Care. 2009;22(7):325–332; quiz 333–334.
7. Clark L, Black J, Black S. Skin tears. In: Capezuti E, Siegler E, Mezy M, eds. Encyclopedia of Elder Care. Second Editon. Springer: New York; 2008.
8. Black J, Gray M, Bliss D, et al. Incontinence-associated dermatitis and intertriginous dermatitis: a consensus. J Wound Ostomy Continence Nurs. 2011; In press.
9. Black J, Edwards K, Cuddigan J, Jizba T, Falcone L. Organisms cultured from sites of intertriginous dermatitis in hospitalized patients: a pilot study. J Wound Ostomy Continence Nurs. 2011; In press.
10. Coloplast Corporation. Inter-Dry®Ag textile provides effective antimicrobial protection against organisms commonly found in skin folds. Coloplast Corporation. Minneapolis MN. 2010; unpublished data.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}