Management of Paraesophageal Hernias in Patients with Morbid Obesity
by Elizabeth Paulus, MD; Aziz M. Merchant, MD; and Edward Lin, DO, FACS
Drs. Paulus and Merchant are from Synergy-Central Michigan University College of Medicine, Department of Surgery, Saginaw, Michigan; Dr. Lin is from Emory University School of Medicine, Department of Surgery, Emory Endosurgery Unit, Atlanta, Georgia.
Funding: No funding was provided for the preparation of this article.
Financial disclosure: The authors report no conflicts of interest relevant to the content of this article.
Abstract
Patients with morbid obesity may be at higher risk than the general population of having paraesophageal or hiatal hernias, presenting a surgical treatment challenge. Repair of large paraesophageal hernias by itself can be associated with high failure rates in the morbidly obese. This article will review the current best evidence involving surgical treatment of this complex patient population, with emphasis on combined approaches of herniorrhaphy and weight loss surgery.
Introduction
Patients frequently present to surgical practices with morbid obesity, a disease that has been shown to be associated with an increased rate of hiatal hernias and gastroesophageal reflux disease (GERD).[1] Hiatal hernias are found more frequently in patients with obesity, and the recurrence rate after repair is higher in patients with morbid obesity than in patients without obesity. The preferred surgical approach to management of hiatal hernia and refractory GERD is laparoscopic hernia reduction, hernia sac resection, crural closure, and possibly antireflux surgery. Although this repair has had excellent success in the general population, Morgenthal et al[1] have shown that fundoplication in the patient population with morbid obesity results in higher rates of failure.
Among hiatal hernias, management of the paraesophageal hernia (PEH) (i.e., hiatal hernia types types II, III, and IV) is probably one of the most debated areas of minimally invasive surgery. The incidence of PEH is rare and is more common in women than in men. PEH often presents in patients during the seventh or eighth decade of life.[2] Both age and the presence of comorbidities increase the risk of repair. The anatomy of the PEH is quite complex. Although rare, PEH can present with a volvulized, strangulated intrathoracic stomach with sepsis, which may cause severe morbidity. Such presentations of PEH allude to the complexity of surgical management of this type of hernia.
Traditional operative management includes sac resection, complete reduction of the stomach into the abdominal cavity, ascertaining adequate intraabdominal esophageal length, hiatal herniorrhaphy with or without patch reinforcement, and possibly some form of antireflux fundoplication and/or gastrostomy tube for stomach decompression.
Routine fundoplication has been traditionally recommended for patients without esophageal dysmotility to prevent reflux and help anchor the stomach in the abdomen.[3]
One of the most challenging presentations of paraesophageal and hiatal hernia repair is concomitant morbid obesity. The prevalence of hiatal hernia and GERD is significantly higher in patients with morbid obesity than in patients without obesity.[4–7] Morbid obesity is a risk factor for recurrence after hiatal hernia repair and antireflux surgery.[1,8] Treatment options for patients with morbid obesity and large PEHs are currently limited to repair of the paraesophageal hernia with or without a concomitant weight loss operation. Options for weight loss operations with PEH repair include laparoscopic adjustable gastric banding (LAGB),[9–11] Roux-en-Y gastric bypass (RYGB),[12,13] and lateral subtotal sleeve gastrectomy (SG).[14]
Each of these three major approaches has theoretical advantages and disadvantages. LAGB concurrently with repair of large PEHs comes with the possibility of band erosions. RYGB concurrently with PEH repair adds significant time and a malabsorptive component for which patients may be unprepared.
Laparoscopic SG does not require as extensive an operation as RYGB and also does not have the malabsorption component. However, SG is also more involved than AGB with a longer gastric staple line.
This review explores and dicusses the evidence for current surgical treatment options for patients with morbid obesity with paraesophageal hernias, with a brief look at the epidemiology, clinical evidence, and future direction in research and surgery.
Epidemiology and Clinical Evidence
Obesity is both a risk factor for developing PEHs and for recurrence once repaired.[8] Moreover, morbid obesity (BMI≥40 kg/m2) has been associated with an increased rate of hiatal hernias, gastroesophageal reflux symptoms, and gastritis.[3,15] GERD has been reported to occur in more than 15 percent of patients undergoing bariatric operations,16 and, indeed, Sharaf et al[17] found a 40-percent occurrence of hiatal hernia on preoperative screening endoscopy prior to bariatric operations. Moreover, Koo et al[18] noted in 2009 that the waist circumference of patients with obesity was associated with erosive esophagitis and hiatal hernia. Therefore, a higher BMI not only puts the patient at risk for reflux disease, but potentially also for the development of adenocarcinoma of the esophagus.[18]
The type of operation performed for patients with PEH depends on the patient’s condition, presence of symptoms, and the category of the hernia. Classification of PEH reveals four subtypes that are determined by the relationship between the gastroesophageal junction,[19] phrenoesophageal ligament and crura, and the gastric fundus. A type I PEH occurs when weakness of the phrenoesophageal ligaments allows the gastroesophageal junction (GJ) to migrate into the chest with a small portion of stomach, commonly referred to as a sliding hiatal hernia. In a type II PEH, the GJ remains at its normal anatomic position, but the fundus of the stomach migrates into the chest cavity. In a type III PEH, both the GJ and the fundus, or body of the stomach, are located in the chest, which is a combination of the type I and type II hernias.
When the sac contains intra-abdominal organs other than the stomach, it is classified as a type IV PEH.
From a biological perspective, a number of investigations have been done on the ultrastructural details of muscle and connective tissue in the setting of hiatal and PEH, and also for obesity. Fei et al[20,21] shows evidence of electron microscopic alteration in the crural muscle of patients with hiatal hernias, although the connective tissue itself did not present any major differences from normal. Using tissue biopsies from the three major hiatal ligaments during antireflux surgery, with or without hiatal hernia repair, Curci et al[22] showed that, compared with patients with GERD alone, the presence of hiatal hernia was associated with a reduction in elastin concentration by more than 50 percent. They concluded that elastin depletion in the periesophageal ligaments links to a structural and biological basis for the development of a hiatal hernia.
Similarly, in an obese Zucker rat study, Biancalana et al[23] concluded that obesity leads to alterations in the composition of extracellular matrix components, and that these alterations might be related to structural rearrangements in collagen bundles that lead to hernia formation. Indeed, obesity is implicated in the problematic remodeling of cardiac extracellular matrix tissues in an obese mouse model under cardiac stress, possibly through a leptin-mediated response,[24] and in poor laparotomy wound healing in obese rats due to abnormal collagen maturation and remodeling.[25] A review of the literature reveals numerous such examples of obesity-related abnormalities of connective tissue and healing, found through human and animal studies.
Recently, Pandolfino et al[26] demonstrated that patients with obesity were likely to have disruption of their GJ (possibly leading to hiatal hernia) based on manometric measurements of the distance between the lower esophageal sphincter and crural diaphragm.
Surgical Options
There are currently no randomized, Level I data that PEH repair with concomitant weight loss procedures lead to better outcomes. However, in the last several years, there have been case series exploring the combined approach to the challenging PEH patient that has morbid obesity. Most of these papers have suggested that hiatal hernia repair in conjunction with a bariatric procedure reduces reflux and hernia recurrences. SG, laparoscopic RYGB, and laparoscopic placement of an AGB have all been described.
There are proven benefits associated with weight loss, including reduction and resolution of certain comorbidities. There still remains controversy regarding which bariatric procedure might provide the best outcome for a patient with morbid obesity and a hiatal hernia. The risks of each approach, such as diarrhea, vitamin deficiencies, and anastomotic leak rate, must be weighed against the benefits. At Emory University School of Medicine, Atlanta, Georgia, our preferred approach is to combine SG because it is less involved than RYGB. It is also acceptable to repair the hernia and stage the weight loss surgery, particularly in cases of reoperative PEH repairs, to reduce operative risks. Nonetheless, whichever bariatric surgery is chosen, it should be combined with traditional good-quality hiatal hernia repair with consideration for mesh reinforcement of the crural closure.
Sleeve gastrectomy. Cuenca-Abente et al[14] described repair of a large, symptomatic, recurrent paraesophageal hernia in a patient with morbid obesity (BMI=46kg/m2) with laparoscopic reduction of the PEH, sac resection, take-down of the prior fundoplication, hiatal closure, and SG. One-and a-half year followup revealed complete resolution of symptoms without recurrence and successful weight loss.
In a comparison with PEH repair with concomitant SG and PEH repair alone (with gastrostomy tube placement), our group at Emory showed that patients with morbid obesity undergoing PEH repair with concomitant SG reported minimal to no symptoms of delayed gastric emptying and required no reoperation, whereas those with gastrostomy gastropexy presented with delayed gastric emptying postoperatively and almost half required some kind of gastric drainage operation due to persistent symptoms.[27] One explanation for this observation may be the effect of SG on gastric emptying and weight loss. Papadakis et al[28] showed a 22-percent increase in gastric emptying after one year in their series of SGs,[28] and this was associated with a significant reduction in BMI. It is possible that the chronically incarcerated stomach in PEH has abnormal gastric motility, and lateral subtotal resection of the stomach helps remove a large part of a relatively defunctionalized cardia and fundus, leaving a narrow, rapidly emptying tube. This would also help decrease the problems with reflux, which were prevalent in the PEH plus gastrostomy group.
The largest reported series to date involving concomitant treatment of hiatal hernia and morbid obesity with laparoscopic hiatal herniorrhaphy and sleeve gastrectomy is that of a subgroup of 15 patients embedded within a larger prospective data collection geared at SG staple line reinforcement.[29] In their repair, after the gastric herniation was reduced into the abdomen, crural reconstruction was achieved with interrupted, pledget-reinforced sutures, with esophageal calibration with a 40 French orogastric bougie. Among the 15 patients, three (20%) had recurrence; one was revised to RYGB, and two awaited reoperation, and there were no other major complications in this subcohort. All patients reported successful concomitant weight loss.
Soricelli et al[30] report a smaller series of six patients with morbid obesity (average BMI 43.4kg/m2) and a hiatal hernia whom underwent a laparoscopic SG and hiatal herniorrhapphy. In their patients, after traditional sac excision and gastric reduction, hiatal closure was achieved with interrupted suture, with hernias greater than 5cm warranting mesh crural reinforcement. Mortality was zero, and there were no peri- or postoperative complications. Median operative time was 90 minutes. Median BMI had fallen to 36.2 four months after the operation. Three of the four symptomatic GERD patients reported symptom resolution, and only one out of six had a small radiologic recurrence.
According to Cuenca-Abente et al,[14] potential advantages of the combined approach include prevention of potential complications, such as gastric volvulus, should the hiatal repair fail, as there is no fundus available for axial rotation, and moderate, safe weight loss associated with a sleeve gastrectomy, as well as all the benefits of a laparoscopic approach. Furthermore, the mass effect of the fundus in the mediastinum and the symptoms associated with it would be prevented if the fundus had been removed. Other case reports with similar outcomes cite similar arguments favoring the laparoscopic SG for concomitant hiatal hernia repair.[31,32] Moreover, emergency sleeve gastrectomy has been described for gastric necrosis due to a strangulated PEH in a women with morbid obesity after AGB.[33]
Adjustable gastric banding. Also described in the literature is simultaneous treatment of morbid obesity and large hiatal hernia with LAGB. It is important to understand that there are conflicting data on the effect of LAGB on GERD. LAGB has been shown to improve GERD symptoms and acid exposure;[34–35] however, it has also been implicated in perpetuating GERD symptoms postoperatively[36,37] Landen11 describes such an operation for a patient with a BMI of 45kg/m2 with a PEH. Anterior and posterior cruroplasties were performed and, after band placement, a posterior crurogastropexy was performed to prevent band and stomach reherniation into the chest. At approximately three-year followup, the patient had a BMI of 36kg/m2 without heartburn or hernia recurrence.
A number of surgeons have shown successful results with LAGB for morbid obesity and standard hiatal hernia. Angrisani et al[9] successfully treated three patients with morbid obesity with concomitant hiatal hernias with standard LAGB and no crural closure. In one patient with a large hiatal hernia, the cruroplasty was performed and the band was deliberately positioned around the esophagus, similar to an Angelchik prosthesis (an incomplete silicon “doughnut” ring, which was a restrictive weightloss procedure) without any postoperative consequences on the esophagus. Anderson et al[10] reported successful management of six patients with morbid obesity, large hiatal hernias greater than 5cm, and reflux esophagitis with LAGB, cruroplasty, and posterior gastrodesis using talc. At six-month followup no major complications were reported. The “pleurodesis” principle was used with talc at the gastric fundus to prevent reherniation or band slippage. In a large series, Dolan et al[38] treated 62 patients with morbid obesity preoperatively screened for a hiatal hernia, by LAGB and routine crural repair. At 14-month followup, median excess weight loss was similar to that of patients without a hiatal hernia who underwent LAGB during the same period. This approach did not increase the risk of slippage or dysphagia but improved reflux symptoms and the need for antireflux medication.
Further, Gulkarov et al[39] analyzed their experience of almost 1,300 patients who underwent LAGB, 520 of which also had a concurrent hiatal herniorrhaphy and crural closure. They showed that patients who underwent concurrent hiatal hernia repair with band placement showed a decreased reoperation rate for band slippage or concentric pouch dilatation. Ramalingam[40] reported a woman with super-obesity (BMI 61.4kg/m2) with a parahiatal hernia (non-hiatal, diaphragmatic hernia) who underwent LAGB and was able to achieve a successful result with concomitant laparoscopic parahiatal hernia repair and LAGB placement.
It is important to note that most studies reporting hiatal hernia repairs with LAGB do not perform the traditional esophageal mobilization, sac excision, and crural closure.
Gastric bypass. RYGB has been performed on patients with morbid obesity and hiatal hernia.
Salvador-Sanchis et al[13] performed a RYGB with concomitant repair of a 7cm PEH and hiatal closure in a patient with morbid obesity (BMI 44.6kg/m2). At six-month followup, the patient achieved a BMI of 31kg/m2 and no hiatal hernia recurrence. Reflux symptoms completely subsided.
Mittal et al[41] reported four patients with morbid obesity in their cohort of patients with PEH. The four patients underwent RYGB; however, no details were reported on the individual outcomes of these four patients.
Khan et al[42] reported the case of patient who presented a number of years after vertical banded gastroplasty with a large, symptomatic PEH, which included the stapled area of the stomach, but with a staple-line dehiscence. The patient successfully underwent repair of the PEH and conversion to a RYGB resulting in resolution of the abdominal pain and weight loss, without recurrence of a hiatal hernia.
The best operation. The question of which operation is best in patients with morbid obesity and a large hiatal hernia is not definitively answered in the current literature. For patients with morbid obesity without PEH, one can turn to a number of large prospective studies and meta-analyses for guidance in comparing AGB and RYGB[43–45] or SG and RYGB[46,47] for resolution of comorbidities. However, a number of technical factors may impact the choice of concomitant bariatric operation with PEH repair.
For example, a patient with prior abdominal surgery and small bowel adhesions may benefit from a SG to obviate the need for a lengthy and complicated abdominal adhesiolysis to access an appropriate length of Roux-limb for a gastric bypass. As a matter of logistic convenience, it seems simpler to perform a SG with a PEH repair because the stomach is already in the surgical field. Placement of a silastic ring or even a band around the stomach warrants greater deliberation because of possible contact of foreign material around weakened serosal surfaces and slippage as points of anchoring are disrupted from the hiatal hernia repair. In general, merely closing the hiatal defect anteriorly without mobilizing the hernia sac is not a hiatal hernia repair. It is also appropriate to repair the PEH, but the surgeon should stage the weight-loss component for 6 to 8 weeks after the initial surgery.
In our experience[27] we have achieved good results with PEH repair, cruroplasty, and reinforcement with SG. We believe that SG allows durable, long-term excess weight loss (EWL) with concomitant excellent comorbidity resolution. Finally, one must remember that part of determining the best operation involves detailed discussion with the patient and his or her family. While it is noble intention to reduce weight as a root cause of morbidity for the patient with PEH, the surgeon should always treat the primary problem first, which is the PEH.
Biologic Patches and Crural Reinforcement
The basic tenets of crural reinforcement after hiatal hernia reduction are 1) establishing excellent visualization, 2) obtaining broad coverage with a patch, and 3) achieving adequate fixation. A number of seminal studies support the use of crural patch reinforcement for hiatal and PEH repair. Gryska and Vernon[48] showed that mesh reinforcement of hiatal cruroplasty is safe, effective, and can be performed without infection and in a tension-free manner. In one of the earlier experiences of patch repair during hiatal herniorrhaphy, Ringley et al[49] compared primary suture cruroplasty with an onlay acellular dermal matrix patch reinforced cruroplasty and found that the latter trended toward reduced hernia recurrence. Several years before, Franztides et al[50] showed similar results with PTFE reinforcement of cruroplasties. In their prospective randomized trial, the primary cruroplasty group had a 22-percent recurrence rate and the PTFE group had none, again showing the ability of biologic patches to achieve successful crural buttressing.[50] Similarly, Granderath et al[51] showed in a randomized study that patch crural reinforcement reduces wrap herniation into the chest in laparoscopic Nissen fundoplications.
Biologic mesh (biomesh) has been proposed as an alternative to conventional mesh products to achieve robust permanent repairs while minimizing stricturing and erosion, theoretically due to less foreign body reaction. Nondegradable synthetic meshes have been associated with serious complications at the hiatus, such as fibrosis, esophageal stricturing, erosion, and gastric fibrosis.[52–54] Using a purely biologic prosthesis, porcine intestinal submucosa (Surgisis, Cook International, Indianopolis, Indiana), to reinforce their cruroplasty during PEH repair, Cuenca-Abente et al14 showed a statistically significant reduction in recurrence rate as compared to nonreinforced, primary cruroplasty (9% vs 24%) at six months. This was one of the earliest Level 1 studies illustrating the efficacy of biologic patches in crural buttressing. Predicting that biologic mesh would result in a higher rate of dysphagia as compared to primary crural repair, secondary to increased inflammation and scar contraction, Goers et al[55] found that by the second postoperative visit the rates of dysphagia were the same and overall complaints were less in the biologic mesh group.
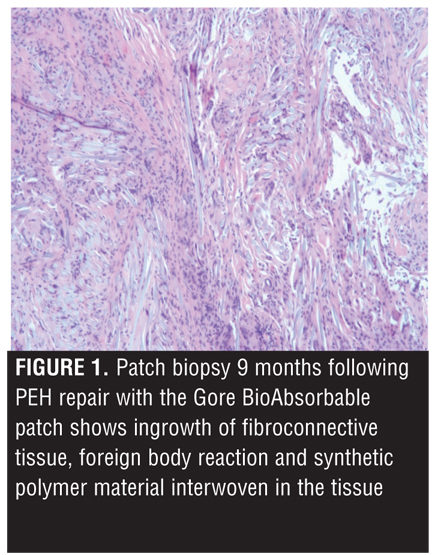
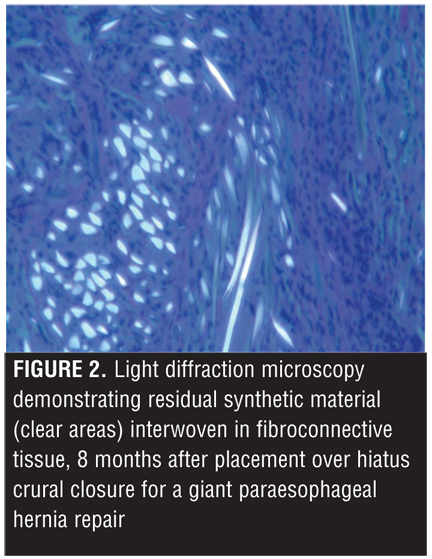
In our study of PEH repair with SG in patients with morbid obesity,[27] biologic mesh derived from porcine intestinal submucosa (Surgisis) was initially used to reinforce our cruroplasty. However, newer synthetic bioabsorbable tissue reinforcement meshes replaced the porcine product. We believe the use of the synthetic bioabsorbable meshes results in a decreased post-operative inflammatory response, possibly due to the fact that it is purely synthetic (i.e., not a xenograft) and is designed to function as a “tissue scaffold” to allow integration of native tissue. Figure 1 and Figure 2 demonstrate histology and immunostaining techniques to this effect. It is possible that this decreased inflammatory response may trigger less scarring, contraction, fibrosis, and stricturing near the hiatus, as described in the complications of prior meshes (synthetic and biologic nonbioabsorbable). The previously mentioned presumptions would, of course, need to be borne out in well-conducted trials; however, the use of biologic synthetic bioabsorbable products for reinforcement of hiatal cruroplasty may well offer advantages over more traditional products.
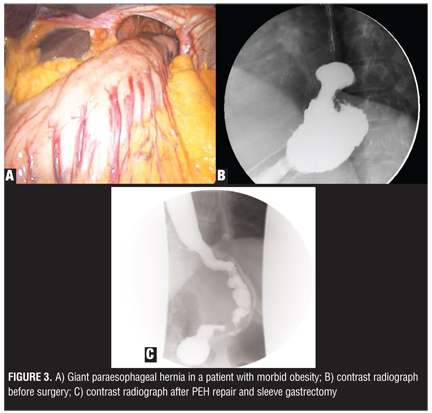
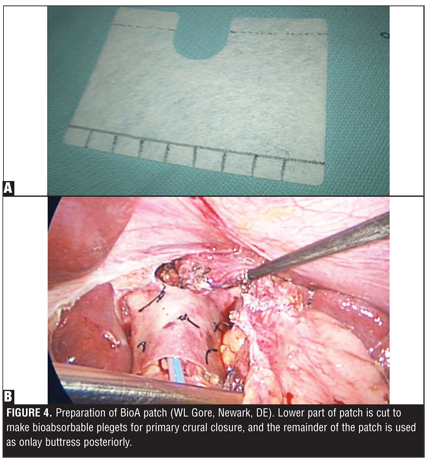
Figure 3 shows the giant hiatal hernia defect in a man with morbid obesity and followup after repair and SG. Figure 4 shows the preparation of the bioabsorbable patch and onlay placement of the patch posterior to the esophagus.
Due to the paucity of data for giant PEH repairs in patients with morbid obesity, we describe our experience for safe management of these patients.27 Steps for safe management are as follows:
1. Fully excise the hernia sac and ascertain adequate intraabdominal esophageal length (endoscopic visualization of the squamocolumnar junction ≥2cm below the hiatus).
2. In reoperative PEH, it is acceptable to delay weight loss surgery for 6 to 8 weeks, depending on the complexity of the PEH surgery.
3. Crural closure should be done over a 56 to 60 French calibrating balloon or bougie.
4. Placement of a drain in the mediastinum may reduce postoperative fluid collection and a mass effect. The drain is certainly appropriate when the pleural cavity is entered, which is not an uncommon occurrence.
5. Current patch reinforcements are not designed to bridge defects, but should be placed over the crura after closure. Sutures or clipping devices have been used to secure the mesh to the crura. We believe tacking devices with screw-anchoring should be used with caution. Whether to encircle the esophagus, use a U-shape patch, or a rectangular patch is a matter of debate. We prefer not to completely encircle the esophagus to avoid dysphagia. We avoid placement of nondegradable and nonbiologic synthetic patches due to the risk of erosion.
6. We follow our patients annually with radiologic studies to monitor for recurrence.
The difficult pEH repair
At times, due to a number of factors, repair of the hernia in the patient with obesity may not be feasible. Lukman et al[56] described emergent repair of a volvulized PEH in a nonagenerian with laparoscopic anterior gastropexy after intra-abdominal reduction of the stomach. Long-term followup was not available, although she was discharged from the hospital in three days. Other series of gastropexy with sac reduction as the sole treatment for a PEH show good outcomes,57 with three out of a series of 13 patients having recurrent symptoms after initial repair. Morbidity and mortality were minimal in this series. In addition, Rosenberg et al[58] presented a series of 21 patients who underwent laparoscopic PEH repair with sac dissection and gastropexy to the anterior abdominal wall, but without an antireflux procedure or repair of the enlarged hiatus. Median length of stay was two days. Two patients required postoperative blood transfusions and one patient had postoperative pneumonia. Three patients had asymptomatic recurrence of PEH at three months postoperatively diagnosed with contrast esophagram, but none of them underwent further surgical treatment.
High-risk patients with obesity with symptomatic PEH may also benefit from endoscopic or laparoscopic assisted gastrostomy tube gastropexy, as illustrated by Jones et al[59] during their retrospective, single-institution review. In their review of five patients whom underwent a laparoscopic-assisted PEG tube placement for incarcerated PEH, there was one mortality. A similar series of 11 elderly, high-risk patients with PEH who underwent flexible endoscopy and PEG gastropexy was reported by Kercher et al in 2001.[60] Average length of stay was 2.8 days with one minor and three major postoperative complications. All patients in that series resumed oral intake and achieved weight gain over a four-month average followup.
In summary, gastropexy without PEH repair appears to be a temporary measure at best with almost certain recurrence or herniation of other visceral organs. In general, when a PEH repair can be performed expeditiously—even without patch reinforcement—the outcomes are better than a gastropexy.
Even when the patient is not high risk, the surgical approach may still be challenging in patients with obesity with large PEH. Rarely are we unable to close at least parts of the crura laparoscopically. It is important to mobilize the esophagus generously so the intraabdominal portion of the esophagus rests comfortably in the abdomen without the need for traction. On occasion, thorascopic mobilization of esophagus through the right chest will free additional esophageal length. Adjuncts to successful hernia closure include lowering the CO2 insufflation pressure to reduce crural tension. We can close the hernia defect posteriorly and anteriorly. While it is tempting to use any of the available patches and bridge the defect gap, most of these patches are designed as on-lay reinforcement over tissue. Lastly, a supradiaphragmatic approach through a thoracotomy is always on reserve to close the defect. In such patients, weight loss surgery can be staged for a later date.
Conclusion
The patient with morbid obesity presenting with hiatal hernia and PEH is a challenge to manage. Although the traditional tenets of hiatal hernia repair apply, the pathophysiology appears to be more complex and demands a well-planned approach based on available evidence in order to achieve the most durable and safe long-term outcomes. The combination of a weight-loss procedure to decrease the risk of recurrence associated with obesity with the traditional components of a PEH repair (without a fundoplication) is emerging as a promising treatment approach to treating patients with morbid obesity with a hiatal hernia. The possibility of an endoluminal approach is in development, which may widen the treatment options for these patients.
References
1. Morgenthal CB, Lin E, Shane MD, et al. Who will fail laparoscopic Nissen fundoplications? Preoperative prediction of long-term outcomes. Surg Endosc. 2007; 21:1978–1984.
2. Davis SS. Current controversies in paraesophageal hernia repair. Surg Clin N Am. 2008; 88:959–957.
3. Casabella F, Sinanan M, Horgan S, Pellegrini C. Systematic use of gastric fundoplication in laparoscopic repair of paraesophageal hernias. Am J Surg. 1996;171:485–489.
4. Dutta SK, Arora M, Kireet A, Bashandy H, Gandsas A. Upper gastrointestinal symptoms and associated disorders in morbidly obese patients: a prospective study. Dig Dis Sci. 2009;54(6):1243–1246. Epub 2008 Oct 31.
5. Wilson LJ, Ma W, Hirschowitz BI. Association of obesity with hiatal hernia and esophagitis. Am J Gastroenterol. 1999;94: 2840–2844.
6. White B, Jeansonne LO, Cook M, et al, Use of endoluminal antireflux therapies for obese patients with GERD. Obes Surg. 2009;19(6):783–787.
7. Menon S, Trudgill N. Risk factors in the aetiology of hiatus hernia: a meta-analysis. Eur J Gastroenterol Hepatol. 2011;23(2):133–138.
8. Perez AR, Moncure AC, Rattner DW. Obesity adversely affects the outcome of antireflux operations. Surg Endosc. 2001;15:986–989.
9. Angrisani L, Iovino P, Lorenzo M, et al. Treatment of morbid obesity and gastroesophageal reflux with hiatal hernia by LapBand. Obes Surg. 1999;9:396–398.
10. Anderson PG, Watson DI. A new surgical technique for the silicone gastric band in the presence of a large hiatus hernia. Obes Surg. 1999;9:202-5.
11. Landen S. Simultaneous paraesophageal hernia repair and gastric banding. Obes Surg. 2005;15:435-8.
12. Zainabadi K, Courcoulas AP, Awais O, Raftopoulos I. Laparoscopic revision of Nissen fundoplication to Roux-en-Y gastric bypass in morbidly obese patients. Surg Endosc. 2008;22:2737–2740.
13. Salvador-Sanchis JL, Martinez-Ramos D, et al. Treatment of morbid obesity and hiatal paraesophageal hernia by laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2010;20(6):801–803.
14. Cuenca-Abente F, Parra JD, Oelschlager BK. Laparoscopic sleeve gastrectomy: An alternative for recurrent paraesophageal hernias in obese patients. JSLS 2006;10:86–89.
15. Loffeld RJLF. Helicobacter pylori, obesity and gastro-oesophageal reflux disease. Is there a relation? A personal view. Neth J Med. 2005; 63:344–347.
16. Ovrebo KK, Hatlebakk JG, Viste A et al. Gastroesophageal reflux in morbidly obese patients treated with gastric banding or vertical banded gastroplasty. Ann Surg. 1998; 228: 51–58.
17. Sharaf RN, Weinshel EH, Bini EJ, et al, Endoscopy plays an important preoperative role in bariatric surgery. 2004;14(10):1367–1372.
18. Koo JS, Lee SW, Park SM, et al. Abdominal Obesity as a Risk Factor for the Development of Erosive Esophagitis in Subjects with a Normal Esophago-Gastric Junction. Gut. 2009;3:276–284.
19. Landreneau RJ, Johnson JA, Marshall JB, et al. Clinical spectrum of paraesophageal herniation. Dig Dis Sci. 1992;37:537.
20. Fei L, del Genio G, Brusciano L, et al. Crura ultrastructural alterations in patients with hiatal hernia: a pilot study. Surg Endosc. 2007;21(6):907–911.
21. Fei L, del Genio G, Rossetti G, et al, Hiatal hernia recurrence: surgical complication or disease? Electron microscope findings of the diaphragmatic pillars. J Gastrointest Surg. 2009 Mar;13(3):459–464.
22. Curci JA, Melman LM, Thompson RW, et al. Elastic fiber depletion in the supporting ligaments of the gastroesophageal junction: a structural basis for the development of hiatal hernia. J Am Coll Surg. 2008;207(2):191–196. Epub 2008 May 19.
23. Biancalana A, Veloso LA, Gomes L. Obesity affects collagen fibril diameter and mechanical properties of tendons in Zucker rats. Connect Tissue Res. 2010;51(3):171–178.
24. Zibadi S, Cordova F, Slack EH, Watson RR, Larson DF. Leptin’s regulation of obesity-induced cardiac extracellular matrix remodeling. Cardiovasc Toxicol. 2011 Jul 10. [Epub ahead of print]
25. Xing L, Culbertson EJ, Wen Y, Robson MC, Franz MG. Impaired Laparotomy Wound Healing in Obese Rats. Obes Surg. 2011 Feb 24. [Epub ahead of print]
26. Pandolfino JE, El-Serag HB, Zhang Q, Shah N, Ghosh SK, Kahrilas PJ. Obesity: a challenge to esophagogastric junction integrity. Gastroenterology. 2006;130(3):639–649.
27. Merchant AM, Cook MW, Srinivasan J, et al, Comparison between laparoscopic paraesophageal hernia repair with sleeve gastrectomy and paraesophageal hernia repair alone in morbidly obese patients. Am Surg. 2009;75(7):620–625.
28. Melissas J, Daskalakis M, Koukouraki S, et al. Sleeve gastrectomy-a “food limiting” operation. Obes Surg. 2008; 18(10):1251–1256.
29. Angrisani L, Cutolo PP, Buchwald JN, et al. Laparoscopic reinforced sleeve gastrectomy: early results and complications. Obes Surg. 2011;21(6):783–793.
30. Soricelli E, Casella G, Rizzello M, et al. Initial experience with laparoscopic crural closure in the management of hiatal hernia in obese patients undergoing sleeve gastrectomy. Obes Surg. 2010;20(8):1149–1153. Epub 2010 Jan 5
31. Varela JE.Laparoscopic biomesh hiatoplasty and sleeve gastrectomy in a morbidly obese patient with hiatal hernia. Surg Obes Relat Dis. 2009;5(6):707–709
32. Korwar V, Peters M, Adjepong S, Sigurdsson A. Laparoscopic hiatus hernia repair and simultaneous sleeve gastrectomy: a novel approach in the treatment of gastroesophageal reflux disease associated with morbid obesity. J Laparoendosc Adv Surg Tech A. 2009;19(6):761–763.
33. Bernante P, Breda C, Zangrandi F, et al. Emergency sleeve gastrectomy as rescue treatment for acute gastric necrosis due to type II paraesophageal hernia in an obese woman with gastric banding. Obes Surg. 2008;18(6):737–741.
34. Dixon JB, O’Brien PE. Gastroesophageal reflux in obesity: the effect of lap-band placement. Obes Surg. 1999;9:527–531.
35. Iovino P, Angrisani L, Tremolaterra F, et al. Abnormal esophageal exposure is common in morbidly obese patients and improves after successful Lap-band system implantation. Surg Endosc. 2002;16:1631–1635.
36. Forsell P, Hallerback B, Glise H, et al. Complications following Swedish adjustable gastric banding: a longterm follow-up. Obes Surg. 1999;9:11–16.
37. Zacharoulis D, Chadhury R, Dobbins B, et al. Laparoscopic adjustable silicone gastric banding: surgical and radiological approach. Obes Surg. 2002;12:280–284.
38. Dolan K, Finch R, Fielding G. Laparoscopic gastric banding and crural repair in the obese patient with a hiatal hernia. Obes Surg. 2003; 13: 772–775.
39. Gulkarov I, Wetterau M, Ren CJ, Fielding GA. Hiatal hernia repair at the initial laparoscopic adjustable gastric band operation reduces the need for reoperation. Surg Endosc. 2008;22(4):1035–1041.
40. Ramalingam G, A D R, T L, H G B. Laparoscopic adjustable gastric banding in a patient with an incidental para-hiatal hernia. Obes Surg. 2006;16(1):98–101.
41. Mittal SK, Bikhchandani J, Gurney O, et al. Outcomes after repair of the intrathoracic stomach: objective follow-up of up to 5 years. Surg Endosc. 2011;25(2):556–566.
42. Khan M, Lee F, Ackroyd R. Revision of vertical banded gastroplasty complicated by a large para-esophageal hernia. Obes Surg. 2010;20(7):960–963.
43. Weber M, Müller MK, Bucher T, et alA. Laparoscopic gastric bypass is superior to laparoscopic gastric banding
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}
{kind=link}