Mesh Fixation Devices and Techniques: A Review of the Literature
Dedicated to providing a venue for interactive exchange of ideas, interesting topics, and surgical pearls from experts in repair of abdominal wall defects as they relate to bariatric surgery
This month’s featured expert
Abraham Fridman, DO, Clinical Fellow, the Bariatric Institute and Section of Minimally Invasive Surgery, Cleveland Clinic, Weston, Florida
Bariatric Times. 2012;9(6):10–12A Message from Column Editor Samuel Szomstein, MD, FACS
Dear Readers of Bariatric Times:
Welcome to the June issue of “The Hole in the Wall.” This issue feature’s Abraham Fridman, DO, Clinical Fellow in Bariatric and Minimally Invasive Surgery at Cleveland Clinic Florida. This month, Dr. Fridman provides us with an excellent literature review on mesh fixation devices and techniques. Do you have any “pearls” or “tricks” that you use in your daily practice related to meshes and fixation devices? Please e-mail it to [email protected], I would love to share it with our readers.
Once again, welcome to “The Hole in the Wall.” We hope you enjoy this column and we look forward to your questions, comments, and participation in future issues.
Sincerely,
Samuel Szomstein, MD, FACS
——
Funding: No funding was provided in the preparation of this article.
Financial disclosures: Dr. Fridman reports no conflicts of interest relevant to the content of this article.
Introduction
Hernia repair has evolved dramatically over the past couple of decades. Since the introduction of prosthetic material (mesh) for hernia repairs, many different techniques have been created to prevent recurrence. With the introduction of laparoscopy for hernia repair, new methods of mesh fixation have been invented. Mesh fixation has evolved from simple sutures to absorbable screw-type fasteners.
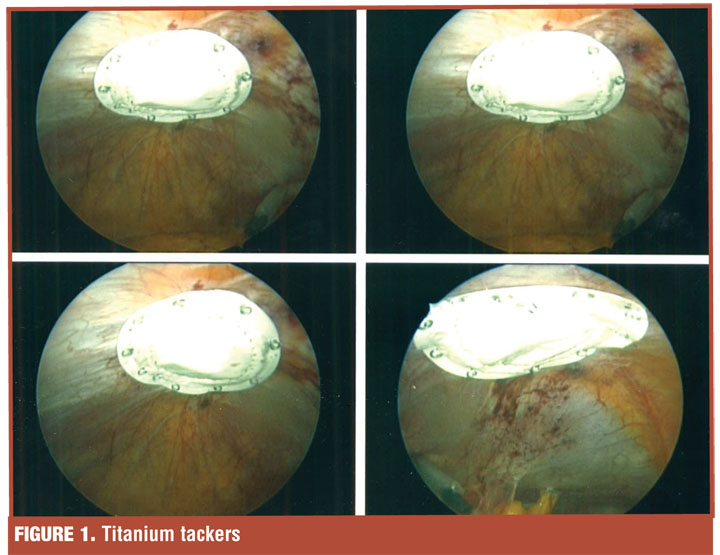
Suture material, non-absorbable or absorbable, was used for hernia repair even before prosthetic materials came around. They are still currently used by many surgeons for open and laparoscopic repairs. One of the first non-suture fixation materials was the titanium tack/staple (ProTack™, Covidien, Norwalk, Connecticut), a permanent spiral fastener, which was a market leader in the early 21st century.
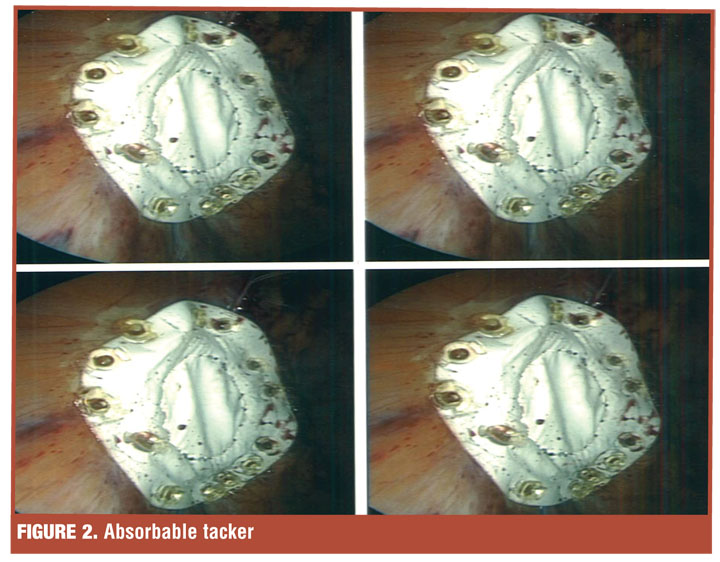
Recently, the market/surgeon preference is turning toward absorbable spiral tacks. These tacks appear to cause less long-term complications than the titanium tacks and tend to reabsorb within one year (as described by the company for the AbsorbaTack). Tissue glues, which for the most part are being used in vascular and cardiothoracic cases, are also being described as an acceptable mesh fixation method. No one fixation material has been shown to be the “ideal” method in the literature. The following is a brief review of current mesh fixation methods and their efficacy.
Ventral/Incisional Hernia
The incidence of incisional hernia after laparotomy has been reported in up to 20 percent of patients.[1,2] Currently, incisional hernias are being repaired by either a laparoscopic or open approach. With neither being accepted as the ideal method of repair, the type of repair is still surgeon dependent.
Laparoscopic repair. Laparoscopic repair has been shown to be aesthetically better than the open approach.[3] Some of the potential pitfalls of laparoscopic hernia repairs include mesh size, mesh fixation, and use of the appropriate mesh type. The main concern in all repairs is to prevent mesh migration and postoperative pain. Many different techniques have been used to fix a mesh during laparoscopic repair.
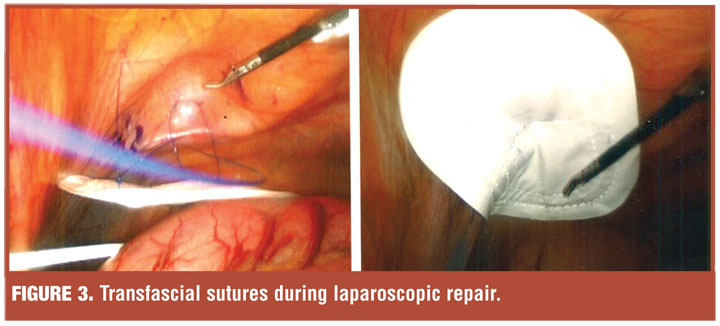
One technique is use of the transfascial suture. Transfascial sutures, using either absorbable or nonabsorbable material, have been shown to have excellent tensile strength, minimal adhesion formation, and minimal cost.[4] A literature review by LeBlanc[4] suggests that recurrence rates are slightly lower when using suture. A group from Israel recently described a new suture passer, which cuts down on the time and significantly simplifies the procedure.[5] Despite the use of this new suture passer, these methods are time consuming, at times difficult to manenuver (suture passer), and have been implicated in being the culprit of chronic pain.[6]
When titanium tacks became available early in the 21st century, they were widely used due to their excellent tensile strength and user friendly application method. With time, surgeons have found them to be associated with bowel injury and very dense adhesion formation in the long term.[2]
Now, newer, absorbable permanent screw fasteners are widely used. These screw fasteners appear to cause the least amount of adhesions and pain, and yet, have enough tensile strength to withstand the body’s movement.[2] In a porcine model, Byrd et al[3] demonstrated that the screw-type devices were associated with decreased adhesions. Lyons et al[7] also recently described barbed anchor sutures for mesh fixation. These sutures are designed to hold tissue without the need for knot tying. This material requires 75-percent less strangulation force and provides adequate fixation; however, no clinical trials have been conclusive.[7]
Open repair. With open repair, there has been no consensus on the ideal fixation method. Surgeons use many different materials and techniques for mesh fixation. In some clinical trials, open repair has been shown to be a better option than the laparoscopic approach.8 Different fixation techniques have been described in the literature. The method of choice varies among different surgeons.
Grommes et al[1] from Germany demonstrated in a pig model that using a retromuscular mesh placement for hernia repair does not require fixation at all. They also concluded that use of a tissue adhesive (BioGlue® Surgical Adhesive, CryoLife, Kennesaw, Georgia) as a mesh fixation method is an adequate method with less complications (pain and seroma) and equal recurrence rates.
Inguinal Hernia
Inguinal (groin) hernias are one of the most common complaints that surgeons hear from patients on a daily basis. With the introduction of prosthetic material for hernia repair, the recurrence rate has dropped Today, groin hernias are managed via a laparoscopic approach with the two most common methods being total extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) repairs. Controversy still surrounds whether laparoscopic or open repair is the ideal for inguinal hernias.
Laparoscopic repair. Mesh fixation for laparoscopic hernia repair, whether TEP or TAPP, remains a widely debated topic. Tackers are very popular fixation devices for inguinal hernia repairs as they are simple to use and prevent mesh migration, which is the most common cause for recurrence.[9,10] However, one of the biggest issues with tacks is the risk of causing long-term pain after its use. In 2008, Taylor et al[11] showed that tacking increases postoperative pain when compared to no fixation. Because of the Taylor et al[11] study, the number of tacks used has dramatically decreased nationwide, with most people only using one or two as adequate fixation.[9,11]
Another method of mesh fixation is using a tissue adhesive material (based on cyanoacrylate or fibrin glue). This method appears to cause less pain than tacks, with equal fixation strength to prevent mesh migration and ultimately recurrence.[10] This method of fixation has been described for both the TEP and TAPP repairs. Brugger et al10 described decreased postoperative hypoesthesia when using tissue adhesive compared to staples, with equal tensile strength and recurrence rates. Whether inguinal mesh needs to be fixed at all is a controversial topic.
Many studies have shown that inguinal mesh fixation adds time to the procedure and may have a higher chance of causing pain, without significantly decreasing recurrence rates. This was described as early as 1999 when Ferzli et al[12] published their experience with no fixation during TEP repair. Also, a recent meta-analysis showed that non-fixation is associated less cost, shorter operative time, and shorter hospital stay.9 Currently, there is no cosensus to the mesh fixation method of choice for inguinal hernia repair.
Open repair. Open approach to inguinal hernia repair remains a very popular technique. The technique has evolved since the incorporation of prosthetic material for repair. Most people still advocate fixing the mesh to the inguinal floor, however, that method is changing. The use of absorbable and nonabsorbable suture material is still widely used. A new and popular method is the self-gripping mesh for inguinal hernias. Self-gripping mesh is made with anchors on one side that adhere to the tissue. Kapischke et al[13] suggested that in this method tensile strength was equivalent to suture fixation with potential decrease in the postoperative pain. Tissue glue has also been proposed as a method for fixation, however no conclusive evidence is available.
Conclusion
Hernias remain one of the most common pathologies seen in the office. The techniques and supplies have been evolving in the recent years. Further clinical trials are needed to determine the optimal technique for hernia repair.
Figures:
Figure 1
References
1. Grommes J, Binnebosel M, Klink CD, et al. Different methods of mesh fixation in open retromuscular incisional hernia repair: a comparative study in pigs. Hernia. 2010;14(6):623–627.
2. Byrd JF, Agee N, Swan RZ, et al. Evaluation of absorbable and permanent mesh fixation devices: adhesion formation and mechanical strength. Hernia. 2011;15(5):553–558.
3. Bansal VK, Misra MC, Kumar S, et al. A prospective randomized study comparing suture mesh fixation versus tacker mesh fixation for laparoscopic repair of incisional and ventral hernias. Surg Endosc. 2011;25(5):1431–1438.
4. LeBlanc KA. Laparoscopic incisional hernia repair: are transfascial sutures necessary? A review of the literature. Surg Endosc. 2007;21(4):508–513.
5. Elazary R, Abu-Gazala M, Schlager A, et al. Trans-fascial laparoscopic mesh fixation: a procedural comparison using the standard suture passer versus iMESH stitcher device. Hernia. 2011;15(3):321–324.
6. Wassenaar E, Schoenmaeckers W, Raymakers J, et al. Mesh-fixation method and pain and quality of life after laparoscopic ventral or incisional hernia repair: a randomized trial of three fixation techniques. Surg Endosc. 2010;24(6):1296–1302.
7. Lyons C, Joseph R, Salas N, et al. Mesh fixation with a barbed anchor suture results in significantly less strangulation of the abdominal wall. Surg Endosc. 2012;26(5):1254–1257.
8. Itani KMF, Hur K, Kim LT, et al. Comparison of laparoscopic and open repair with mesh for the treatment of ventral incisional hernia. Arch Surg. 2010;145(4): 322–328
9. Teng YJ, Pan SM, Liu YL, et al. A meta-analysis of randomized controlled trials of fixation versus nonfixation of mesh in laparoscopic total extraperitoneal inguinal hernia repair. 2011;25(9):2849–2858.
10. Brugger L, Bloesch M, Ipaktchi R, et al. Objective hypoesthesia and pain after transabdominal preperitoneal hernioplasty: a prospective, randomized study comparing tissue adhesive versus spiral tacks. Surg Endosc. 2012;26(4):1079–1085.
11. Taylor C, Layani L, Liew V, et al. Laparoscopic inguinal hernia repair without mesh fixation, early results of a large randomized clinical trial. Surg Endosc. 2008;22(3):757–762.
12. Ferzli GS, Frezza EE, Pecoraro AM Jr, Ahern KD. Prospective randomized study of stapled versus unstapled mesh in a laparoscopic preperitoneal inguinal hernia repair. J Am Coll Surg. 1999;188:461-465.
13. Kapischke M, Schulze H, Caliebe A. Self-fixating mesh for the Lichtenstein procedure-a prestudy. Langenbecks Arch Surg. 2010;395(4):317–322.
Category: Hole in the Wall, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}