Surgical Pearls: The Intragastric Balloon Procedure
Surgical Pearls: Techniques in Bariatric Surgery
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS, and Daniel B. Jones, MD, MS, FACS
This Month’s Technique: The Intragastric Balloon Procedure
This Month’s Featured Experts:
Gontrand Lopez-Nava, MD
Bariatric Endoscopy Unit, Madrid Sanchinarro University Hospital, Madrid, Spain
Nicole Peña, MD
Clinical Professor of Medicine, Universidad Pedro Henriquez Urena (UNPHU), Santo Domingo, Dominican Republic
Natan Zundel, MD, FACS, FASMBS
Clinical Professor of Surgery, Vice-Chairman Department of Surgery at Florida International University, Herbert Wertheim College of Medicine in Miami, Florida
Funding: There was no funding for the preparation of this manuscript.
Disclosures: Dr. López-Nava has acted as an independent consultant for ReShape Medical, San Clemente, California. Dr. Zundel has acted as a consultant for Apollo Endosurgery, Inc., Austin, Texas. Dr. Peña has acted as a proctor for Apollo Endosurgery, Inc., Austin, Texas.
Bariatric Times. 2015;12(10):8–9.
Introduction
The desire to lose weight is expanding among not only individuals with obesity (body mass index [BMI] ≥30kg/m2) and morbid obesity (BMI ≥ 35kg/m2), but also those who are overweight (BMI of 25.0–29.9kg/m2) and are affected by comorbidities, such as as type 2 diabetes mellitus (T2DM) and hypertension.[1]
The intragastric balloon (IGB) has been developed as a temporary and reversible therapeutic option for treatment of obesity. It is potentially attractive to healthcare practitioners who have experienced poor results with dietary programs, drug treatment, and behavioral therapy,[2] or have patients who decline surgery.
Currently, two intragastric balloon systems are approved for use in the The ORBERA™ Intragastric Balloon System (Apollo Endosurgery, Inc., Austin, Texas) is a weight-loss system that uses a single gastric balloon. The ReShape™ Integrated Dual Balloon System (ReShape Medical, Inc., San Clemente, California) is a weight-loss system that uses two attached balloons that are filled and sealed separately. Both systems work by occupying space in the stomach, thus creating a feeling of fullness in the patient. The products are placed into the gastric cavity through the mouth, during a minimally invasive endoscopic procedure, while the patient is under mild sedation.
The procedure requires rigorous patient selection and close follow up by a multidisciplinary team working with behavioral and nutritional habit modification program to achieve good long-term results.
Upper endoscopy is required for balloon placement. This can be done under conscious sedation (propofol 2–3mg/kg) or general anesthesia with orotracheal intubation (in patients with BMI>40kg/m2, with obstructive sleep apnea or chronic obstructive pulmonary disease).
First day’s tolerance can be challenging, patients can expect discomfort, nausea/vomiting, and abdominal pain.
Although the deflation rate with concurrent bowel migration is very low, it should be considered during the six-month period in which the balloon should maintain an intragastric location. After this period the balloon has to be explanted. The explantation process also uses upper endoscopy and conscious sedation or orotracheal intubation, which we highly recommended.
After balloon placement or removal, patients may be discharged from the hospital or clinic in 2 to 3 hours.
Currently, studies show that IGB procedures are safe with a very low rate of complications and also effective with an average reported weight loss of 26.5 to 50 pounds.[3]
Preoperative Workup
First, we review the patient’s medical history, psychological evaluation, blood tests, and upper diagnostic endoscopy report. We look for anything that would exclude them from undergoing the procedure, including pregnancy and inflammatory or potential upper gastrointestinal bleeding conditions. We also assess whether patients are willing and able to commit to the follow up and lifestyle changes. Only patients who have been deemed eligible are scheduled for the procedure.
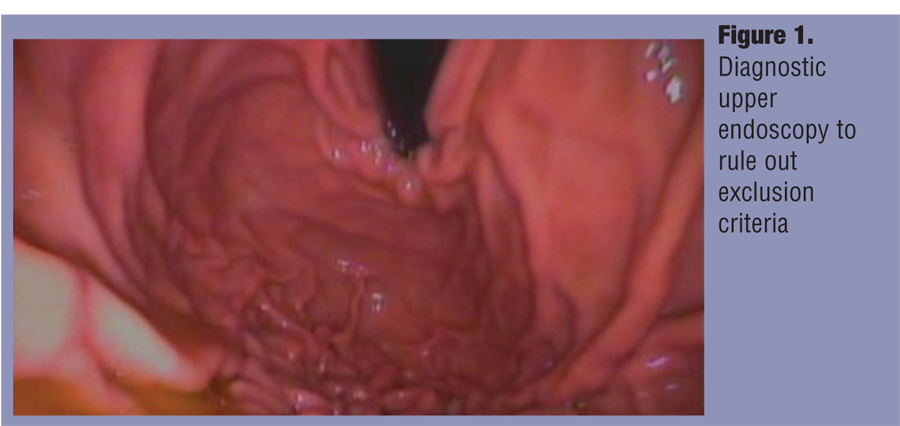
Step 1: Diagnostic upper endoscopy. The patient is required to undergo an upper diagnostic endoscopy in order to rule out potential bleeding lesions (ulcers, erosions, gastritis, esophagitis), gastric mass, hiatal hernia measuring more than 5cm., and/or signs of prior gastric surgery (Figure 1).
Step 2: Intragastric balloon insertion. A deflated IGB is inserted under direct vision via endoscopy and pushed by the insertion catheter with a guide wire inside to stiffen the balloon and carry it to lay in the greater curvature and below the gastroesophogeal (GE) junction (Figure 2).
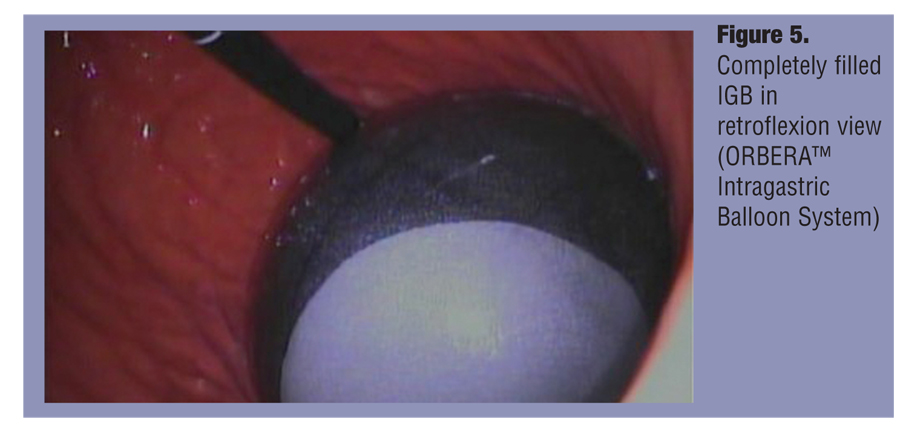
Step 3: IGB filling. After removing the internal guide wire of the catheter, the balloon is filled up to a volume between 500 and 700mL of saline using a 60mL Luer syringe or an endoscopic pump. All steps are performed using direct endoscopic vision. Once the desired final volume is achieved, the catheter can be detached by simply pulling it (Figure 3, Figure 4, Figure 5).
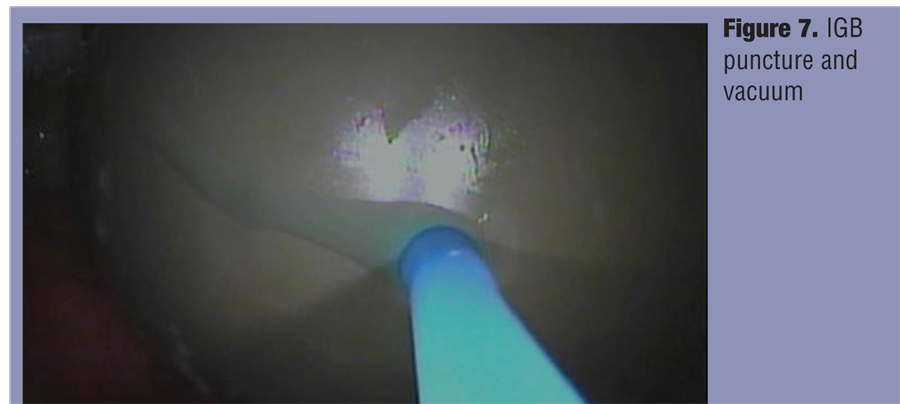
Step 4. Removal. Puncture and deflation of the IGB. Orotracheal intubation is recommended for balloon removal to protect the airway from any aspiration of alimentary fluid or acid dripping from the balloon. A strict gastric emptying protocol is recommended 48 hours before the patient is due to undergo the balloon removal procedure.
With the patient in the left lateral position, we introduce the scope with the extraction needle in the working channel to perforate the balloon and to suction the saline with a central vacuum or a pump until the IGB is completely deflated (Figure 6 and Figure 7).
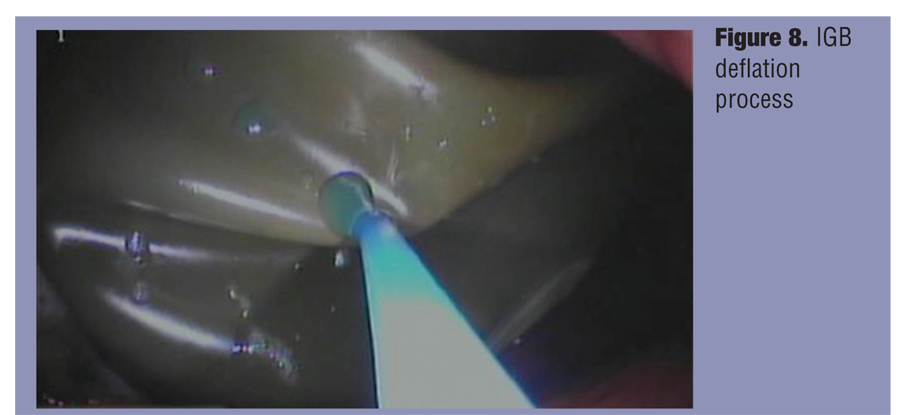
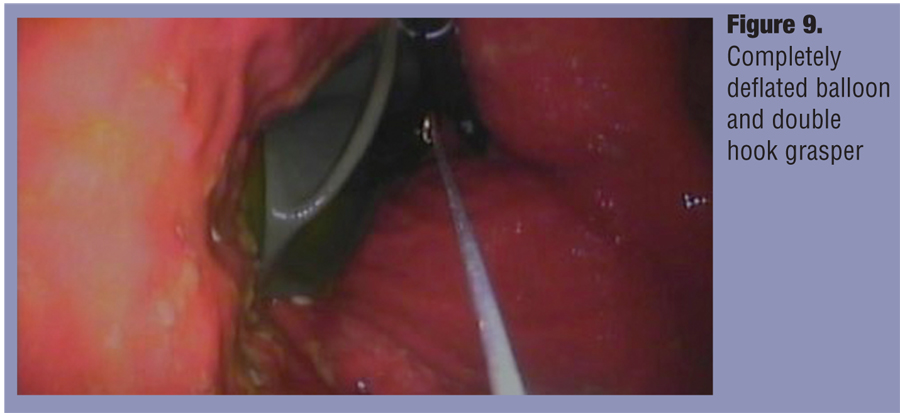
Step 5. Removal. Grasping of the IGB. The balloon should only be grasped when it is throughly contracted and devoid of any internal saline. We grasp the balloon using a double inverted hook grasper from the proximal part in anterograde view or from the distal in retroflexion (Figure 8 and Figure 9). We recommend the latter.
Figure 10 shows Feature at the tip of the ReShape™ Integrated Dual Balloon System that enables grasping.
Figure 11 shows IGB grasping.
Conclusions
The IGB for the treatment of obesity is a simple and feasible procedure for trained doctors, with a a learning curve that is easily mastered. In conjunction with a multidisciplinary follow up, we find that it is an effective tool for weight loss in patients who are willing and able to commit to a behavior modification program to obtain long-term lifestyle changes.
The data show that with the proper placement and removal technique and comprehensive follow up, the rate of complications are low and the treatment is safe. IGB can be considered as part of the arsenal we can offer patients to treat weight-related issues.
References
1. Genco A, López-Nava G, Wahlen C, Maselli R, Cipriano M, Sanchez MM, et al. Multi-centre European experience with intragastric balloon in overweight populations: 13 years of experience. Obes Surg. 2013;23(4):515–521.
2. Genco A, Balducci S, Bacci V, et al. Intragastric balloon or diet alone? A retrospective evaluation. Obes Surg. 2008;18(8):989–992.
3. Lopez-Nava G, Rubio MA, Prados S, Pastor G, Cruz MR, Companioni E, Lopez A. BioEnterics® intragastric balloon (BIB®). Single ambulatory center Spanish experience with 714 consecutive patients treated with one or two consecutive balloons. Obes Surg. 2011;21(1):5–9.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}