The Medical Student Notebook: Bariatric Physiology
This column is written by medical students and is dedicated to reviewing the science behind obesity and bariatric surgery.
Lesson #1 explores topics in gastrointestinal physiology and discusses the implications of gastric bypass surgery for each subject.
Column Editor: Daniel B. Jones, MD, MS, FACS
Professor of Surgery, Harvard Medical School
Vice Chair, Beth Israel Deaconess Medical Center
Boston, Massachusetts
Featured Student: Kyle D. Checchi, MSc
Medical Student, Harvard Medical School, Boston, Massachusetts
This month: Lesson #1: Bariatric Physiology
Part 2: Bariatric Surgery and Iron
by Kyle D. Checchi, MSc
Bariatric Times. 2014;11(6):14–15.
Introduction
Lesson #1 of The Medical Student Notebook is a five-part series focused on gastrointestinal physiology. Part 1, published in Bariatric Times March 2014, discussed bariatric surgery and B12. In Lesson #1, Part 2, we examine bariatric surgery and iron.
Part 2: Bariatric Surgery and Vitamin B12
Iron is a critical element to the function of all tissues, most notably erythrocytes and myocytes.[6] Considering iron’s vital importance, it is not surprising that the body has developed an intricate mechanism to facilitate and regulate its absorption. Dietary iron comes in two forms, elemental or bound as heme, in various proportions depending on one’s diet.[6] These two forms of iron are absorbed in slightly different fashions.
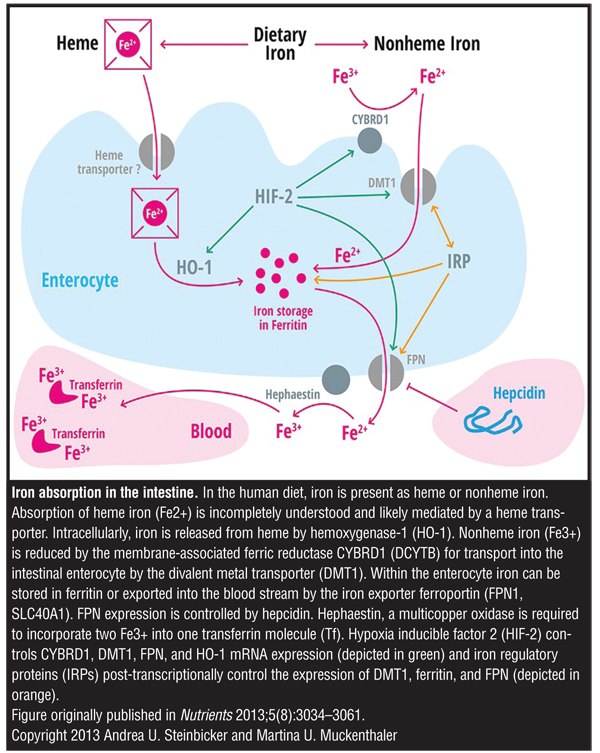
For elemental iron, the acidic environment of the stomach and proximal duodenum help to solubilize elemental iron, making it available for absorption.[6] The brush border enzyme duodenal cytochrome B reduces solubilized ferric 3+ iron to ferrous 2+ iron, which can be absorbed into the luminal cell through a divalent metal transporter (DMT1).[7] Within the cell, the 2+ iron is either directed to the cytoplasm through ferroportin 1 transporters where it is oxidized and bound to transferrin or stored within the luminal cell bound to ferritin depending on the presence and availability of ferroportin transporters, which is governed by circulating hepcidin levels according the levels of intrahepatic iron.[7]
Heme iron is directly absorbed from the gut into lumninal cells through a separate and not well characterized heme transporter on the apical surface. The heme is then internally metabolized within the luminal cell into elemental 2+ iron, where it joins the classical pathway.[7]
Gastric bypass has many impacts on this elegant process of iron absorption. First, gastric bypass reduces the intake of dietary iron through restriction.[8] Second, reduced stomach lumen surface area, reduced stomach retention capacity, and anti-acid therapy limit the extraction and solubilization of iron from the diet.[8] Lastly, the duodenum is almost completely or completely bypassed in the biliopancreatic diversion with duodenal switch and Roux-en-Y procedures, bringing iron to distal segments of the alimentary canal and shortening the overall length of the digestive tract.[8] However, despite these disruptions to the multistep process of iron absorption, a surprising number of bariatric patients manage to maintain adequate iron metabolism with only 6 to 50 percent of patients developing iron deficiency.[8]
The number of bariatric patients with adequate iron absorption is explained by numerous factors. The main protection comes from the body’s handling of iron that has already been absorbed. Iron is tightly bound within the body and has no mechanism of natural excretion apart from blood loss and sloughing of the skin and luminal digestive surface.[6] This tight hold on absorbed iron minimizes the amount of iron that needs to be replaced. Additionally, the ileum and jejunum may not be able to up-regulate their absorption as well as the duodenum, but they can still absorb some iron, ideally enough to overcome the minimal iron losses.[8] Lastly, iron can be supplemented in the diet, including through solubilized iron preparations that can bypass the body’s impaired solubilization capacity.[6]
Iron absorption in the intestine
This second installment of Lesson #1 in the Medical Student Notebook shows again that understanding the basic principles of physiology can help physicians understand the underlying causes of particular nutritional deficiencies following gastric bypass, and can also help inform the approach to patient care. For example, by understanding the mechanisms by which bariatric surgery reduces the ability of the body to extract and absorb iron, nutritional counseling about seeking good dietary sources of iron such as meat rather than vegetables, preventing the inhibitory effects of phytates and phosphates in many foods by taking tablet supplements on an empty stomach, and the use of solubilized preparations in refractory cases can minimize the prevalence of iron deficiency in bariatric surgery patients.[6]
References
1. Wang YC, McPherson K, Marsh T, et al. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet. 2011;378(9793):815–825.
2. Brolin RE. Bariatric surgery and long-term control of morbid obesity. JAMA. 2002 11;288(22):2793–2796.
3. Desjeux JF. The molecular and genetic base of congenital transport defects. Gut. 2000;46(5):585–587.
4. Furness JB. The enteric nervous system and neurogastroenterology. Nat Rev Gastroenterol Hepatol. 2012;9(5):286–294.
5. Xanthakos SA. Nutritional deficiencies in obesity and after bariatric surgery. Pediatr Clin North Am. 2009;56(5):1105–1121.
6. Longo DL, Fauci AS, Kasper DL, et al. Harrison’s Principles of Internal Medicine. 18th Edition, Volume 2. McGraw-Hill Professional; 2012.
7. Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran Pathologic Basis of Disease. Professional Edition: Expert Consult-Online. Saunders, an imprint of Elsevier Inc., Philadelphia, PA; 2009.
8. Love AL, Billett HH. Obesity, bariatric surgery, and iron deficiency: true, true, true and related. Am J Hematol. 2008;83(5):403–409.
FUNDING: No funding was provided for this article.
FINANCIAL DISCLOSURES: The authors report no conflicts of interest relevant to the content of this article.
Category: Medical Student Notebook, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}