Trends in the Perception of Obesity
NEW COLUMN: The Mentored Student Clinical Casebook
First year medical students at Harvard Medical School are paired with a faculty member and a patient for the year. The student assignment is to go to all of the information sessions, and preoperative, introperative, and postoperative appointments. This column is a collection of the essays written by medical students on a topic of their choice at the end of this experience.
Column Editor: Daniel B. Jones, MD, MS, FACS
This month: Trends in the Perception of Obesity
by Raaj S. Mehta, AB
Bariatric Times. 2012;9(5):18–20
Funding: No funding was provided in the preparation of this manuscript.
Financial disclosures: The author reports no conflicts of interest relevant to the content of this article.
Introduction
Obesity is a uniquely public disease. Unlike nearly any other illness, it is simultaneously a visible condition as well as a health topic that is nearly inescapable in the United States because of coverage it receives from the news media.[1] Therefore, many of us already know that American waistlines are rapidly expanding, and have heard that the prevalence of obesity has dramatically increased from 23 percent in 1994 to 34 percent in 2008.[2] It is also little surprise that the rapid increase in weight has tremendous implications for human health.
But, do we know exactly what the term obesity means, and what its different severities are?
Many patients describe obesity simply as “being very fat,” which isn’t far from the technical definition provided by the World Health Orgization (WHO) that defines obesity as a condition of excess fat accumulation in adipose tissue, to the extent that health may be impaired.3 The descriptions of “very” and “excess” used in these definitions can be interpreted in an infinite number of ways, thus, the WHO further explains that obesity can be defined using the body mass index (BMI). Categories of obesity as defined by BMIs are as follows:[4]
• Overweight: BMI 25.0–29.9kg/m2
• Class I obesity: BMI 30–34.9kg/m2
• Class II obesity: BMI 35–39.9kg/m2
• Morbid obesity: BMI 40–44.9kg/m2
• Super obesity: BMI≥45kg/m2
Armed with these specific and quantitative definitions, it theoretically should be easy to recognize the difference between an overweight person and an obese person, or the difference between morbid and severe obesity. After all, unlike with bone fracture, one can use a table on the back of a cereal box to compute a BMI, which enables us to clinically assess health risks.
In this Casebook, I will discuss perceptions of obesity to show that a significant and increasing proportion of the United States population does not have a firm understanding of how to recognize obesity. I will also state why this is a problem, propose some reasons for why more people are misperceiving their own obese/overweight status, and conclude with ways we can address this issue. Perception in obesity is an understudied topic in the treatment of obesity and, if better understood, could have tremendous implications for the epidemic.
Obesity: A Visible Condition?
For the Mentored Clinical Casebook Project (MCCP), I was assigned to the Beth Israel Deaconess Bariatric Center in Boston, Massachusetts. For the first two months, I attended information sessions, met the center’s team, and prospective patients (all of whom had BMIs≥40kg/m2). Though I knew all were considered to have morbid obesity, I still found myself wondering why some showed up, because they didn’t seem so “fat” to me. Certainly, baggy and black clothing masks folds of fat much better than skin-tight jeans, but I began to pick up on more subtler differences. For example, people with a lot of weight in their face, especially in the neck and arms, were easily classifiable as obese, from my perspective. On the other hand, for those who had all of their weight in their abdominal region or in their thighs, it was harder to say whether they were indeed morbidly obese or just overweight. As a result, I began to wonder if there is a subconscious distinction made by people between “normally” obese and “pathologically” obese, and if we judge obesity as a sum of one’s body parts rather than viewing the whole person.[1] These experiences prompted me to learn more about the perceptions of obesity.
In November 2011, I was preparing to greet my patient, Susan, for the first time, but when I stepped out into the laparoscopic surgery waiting room, I couldn’t pick her out from the other 20 people around her. Not everyone was waiting for the weight loss clinic, of course, but I still found it difficult to say who was morbidly obese and who wasn’t; who was waiting for the bariatric surgeon and not for a gallbladder removal. Interestingly, a week after my patient and I did connect, she confessed that she never saw herself as morbidly obese when looking in the mirror. She knew she was overweight and that her BMI was 43kg/m2, but she “always thought that gastric bypass was for really fat people.” It wasn’t until her mom who was a nurse gave her “a reality check” that she began to explore surgical interventions. Her perception of obesity, like mine, was off, and her BMI number ultimately meant very little for her body image.
Misperceptions of Obesity
Society past and present. Our country has historically ridiculed individuals with obesity. During the Gilded Age, an era not too different from our own, people with morbid obesity were considered “freaks” and were touted around on tour in circuses alongside men with extra limbs or women with abnormal facial hair.[5] Furthermore, our condemnation of obesity as of late has led to serious public health-related body image problems. For example, Western society in recent decades has promoted images of unhealthily thin women. Many lament today that from 1922 to 1999, Miss America has lost 12 percent of her weight while gaining two percent height.[6] And now, evidence is emerging that objectification of men is creating new obsessions with exercise and perhaps unnaturally muscular body types.[7]
Emerging evidence. Recognizing obesity. Despite the stigma associated with obesity, it appears that misperceptions of obesity and overweight are not uncommon. According to recent evidence, 50 percent of men fail to self-classify themselves as having obesity (as determined by BMI). This trend is also high among African Americans and Hispanics.[8] For example, among more than 2000 subjects with obesity from the Dallas Heart Study, eight percent of those surveyed failed to recognize their correct weight status. In the same study, 14 and 11 percent of the African American and Hispanic population, respectively, were found to be significantly more likely to misperceive their true weight.[9] Moreover, the prevalence of cardiovascular effects in this subset with body size misperception was comparable if not worse than the rest of the group.[9]
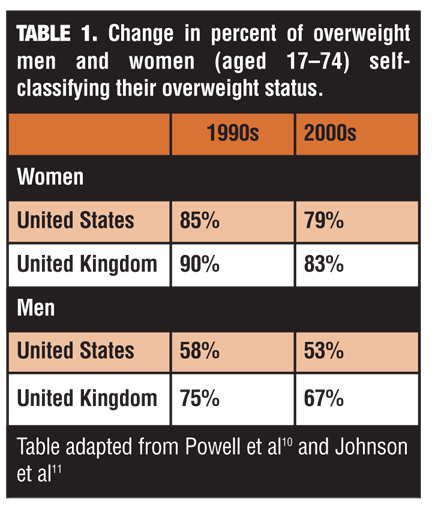
Two landmark reports in the British Medical Journal[10] and Obesity[8] revealed that over the course of a decade, significantly fewer people are correctly identifying themselves as obese or overweight. In the United States, data from The National Health and Nutrition Examination Survey (NHANES) cohorts showed that from the period 1988 to 1994 to the period 1999 to 2004, the proportion of overweight women (as indicated by BMI) reporting that they were overweight fell by six percent. Recognition of overweight similarly fell by about five percent in the male population. Likewise, from 1999 to 2007 in the United Kingdom, recognition of overweight status in overweight men and women fell by eight and seven percent, respectively (Table 1).[9,10]
Most striking of these results is that young people saw the biggest decline in the recognition of obesity. In the United States, there was an eight-percent decrease in accurate self-classification by female subjects with obesity aged 17 to 19 and an 11.5-percent decrease among men with obesity in the same age range.[8] This subgroup also saw the largest increases in average BMI and adult obesity.8 In addition, a study from 2010, found that nearly 1 in 3 high school students in the United States who have overweight or obesity think they are at a normal weight.[11]
It may seem obvious that these trends are disconcerting and should be addressed. After all, it is supported by evidence that increased perceptions of being overweight will lead to weight loss attempts for both genders.[12]
Obesity and Mental Health
Some studies have shown that those who constantly feel pressured to shed excess weight are actually less healthy than those who have obesity and are happy.[13] People who reported being satisfied with their weight, despite being overweight or obese, had fewer physically unhealthy days and fewer mentally unhealthy days compared to people who were unhappy with their weight, when controlling for BMI.[13] Furthermore, while it is believed that some level of dissatisfaction can be productive to encourage weight loss and motivate healthier behavior, the benefits follow a negative parabolic curve. Evidence shows that too much distress about one’s body image can lead to increased eating, due to psychological reasons.[14]
My MCCP patient certainly experienced this vicious cycle. Initially, her frustration with her weight led her to join a gym and start walking her dogs. Eventually, though, her determination became depression, which worsened as she gained more weight. The weight gain and depression combined encouraged her to binge eat more than ever.
The stress that one experiences when intensely dissatisfied with one’s body image can lead to a permanent state of depression. Dr. Hatchigian, a bariatrician at the Beth Israel Bariatric Center, commented: “Even after surgery, after losing 100, 150, or 200 pounds, many of our patients come in and still think they’re obese. I have to convince them—by showing them on the chart how much weight they’ve lost—that the procedure worked.”
This phenomenon has been termed in the literature as phantom fat, and it has been repeatedly observed that people who work hard to lose their excess fat never gain the same positive body image as someone one initially satisfied with their weight, regardless of how much weight is lost.[14]
Despite these findings, I don’t think there should be any excuse to not address obesity appropriately and understand these misperceptions. Surely while we can do a lot to promote a healthy body image, condoning obesity is not the only solution. Given that anorexia and bulimia levels seemed to have stabilized,[15] and the knowledge that obesity is a major contributor to cardiovascular and metabolic disease development, I believe that we should actively explore why this increasing misperception phenomenon is occurring.
Possible Causes of Misperception
Social comparison hypothesis. The first explanation for the observed increase in misperception of obesity is the “social comparison hypothesis,” made popular by the seminal paper by Christakis and Fowler.[16] Essentially, they found that social networks seem to facilitate the spread of obesity, irrespective of geographical distance. Thus, as the number of people with obesity in one’s social circle increases, it becomes more and more acceptable to be obese, or obesity becomes more normalized. This theory is corroborated by recent survey data that show that ideal body weight in the United States is steadily creeping upward.18 Women believe their ideal weight should be 138 pounds, up from 129 pounds in 1991. Men stated that their ideal weight should also be greater, at 181 pounds instead of 171 in 1991.[17] The social comparison hypothesis might also help explain the peculiar differences in male versus female recognition of obesity. Perhaps because there are significantly more men in the United States who are obese compared to women (71.2% versus 57.0%),[18] it might be more “normal” for a man to be obese since more of his peers also have obesity. Finally, if the social comparison hypothesis holds true, and if the establishment of body image norms occurs largely during childhood, the increase in childhood misperception of weight class holds grave implications for the future prevalence of obesity.
Societal forces. While the social comparison theory applies to those close to an individual, I believe that there must also be some larger societal pressure that can come from even those irrelevant to you. Regardless of how closely clustered together people are and how homogenous a neighborhood or social circle is, you invariably feel the effects of the media on you, and other societal forces. There is no clearer example of this than in Anne Becker’s research, which showed that even thousands of miles away, Fijians were affected by the anti-fat bias of a culture.[19] If anything, the Fijians in this study seemed to be more vulnerable to United States cultural propaganda than its citizens.
If there is some larger societal effect, wouldn’t we expect a decrease in misperception as the anti-fat bias continues to permeate society? My thought, though largely unsubstantiated, is that perhaps there is a significant pro-fat bias these days. The first, though perhaps unintentional, is due to the “healthy image” campaigns on TV and even in schools, which were supposed to reduce the amount of anorexia and eating disorders.[8] It is entirely possible then that these are contributing to children feeling better about their body weight, even though they are overweight or obese, which then leads to later adult obesity. Furthermore, it is possible that the media is focusing on only the severely obese during news segments, and thus some have come to believe, like my patient Susan, that they are fine if they don’t look like “one of those people”[8] Finally, perhaps with knowledge that treatment and care for chronic diseases like diabetes and cardiovascular disease has improved, people are more cavalier about their health, and are less willing to change their behavior.
Final Thoughts
There is much to be done to curb the rise of obesity in our country and abroad. Great strides could be made if our environment were less obesogenic, an issue that others are already working to hard to address.[21] In order to specifically reduce the rate of misperception of obesity, however, we may need to turn to primary care. The data presented in Table 1 shows that while both the United Kingdom and the United States are experiencing increases in misrecognition of obesity, self-recognitions rates are higher in the United Kingdom than in the United States. This could be due to any number of factors, but perhaps one of the biggest differences between the two countries is access to primary care in the United Kingdom because of the national health insurance system. This theory is supported by an article published in the New England Journal of Medicine that found that “enhanced lifestyle counseling” in the primary care setting helps one-third of patients to lose significant amounts of weight.[21] Furthermore, a simple diagnosis of obesity by a primary care physician—something that Dr. Hatchigian notes he rarely sees—will more likely result in an action plan and weight loss.[22] This is especially important for the recognition of childhood obesity, since only one-quarter to one-third of parents have been reported to recognize overweight or obesity in their children.[23]
The beauty and tragedy of medicine is that there are innumerable factors that contribute to the etiology of a disease. What is undeniable, though, is that recognition of obesity and its misperception is a critical issue that affects millions of people in the United States and abroad and should be studied more, be it through social network interactions; continued surveys; or even at the biochemical, physiological, and genetic level.
References
1. Badger S. Abject bodies: Where excess grows. In: Ettorre E, ed. Culture, Bodies and the Sociology of Health. Liverpool: Ashgate Publishing; 2010: 137.
2. Ogden CL, Carroll MD. Prevalence of overweight, obesity, and extreme obesity among adults: United States, trends 1960–1962 through 2007–2008. CDC June 2010. http://www.cdc.gov/nchs/data/hestat/obesity_adult_07_08/obesity_adult_07_08.htm. Accessed 12/08/2011
3. World Health Organization. Obesity and overweight. Fact sheet N°311. March 2011. http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed 12/08/2011
4. Hamdy O, Citkowitz E, Uwaifo G, et al. Obesity. Medscape Reference, November 8, 2011. http://emedicine.medscape.com/article/123702-overview. Accessed 12/08/2011
5. Mitchell M. Monsters: Human Freaks in America’s Gilded Age: The Photographs of Chas Eisenmann. Toronto: ECW Press; 2002.
6. Rubinstein S, Caballero B. Is Miss America an undernourished role model? JAMA. 2000;283(12):1569.
7. Parent MC, Moradi B. “His biceps become him: a test of objectification theory’s application to drive for muscularity and propensity for steroid use in college men. J Couns Psychol. 2011;58(2):246–256.
8. Burke MA, Heiland FW, Nadler CM. From “overweight” to “about right”: evidence of a generational shift in body weight norms. Obesity (Silver Spring). 2010;18(6):1226–1234. Epub 2009 Oct 29.
9. Powell TM, de Lemos JA, Banks K, et al. Body size misperception: a novel determinant in the obesity epidemic. Arch Intern Med. 2010;170(18):1695–1697.
10. Johnson F, Cooke L, H Croker, and J Wardle. Changing perceptions of weight in Great Britain: comparison of two population surveys. BMJ. 2008;337:a494.
11. Edwards NM, Pettingell S, Borowsky IW. Where perception meets reality: self-perception of weight in overweight adolescents. Pediatrics. 2010;125(3):e452–e458. Epub 2010 Feb 8.\Continued from page 20
12. Lemon SC, Rosal MC, Zapka J, et al. Contributions of weight perceptions to weight loss attempts: differences by body mass index and gender. Body Image. 2009;6(2):90–96. Epub 2009 Feb 1.
13. Muennig P, Jia H, Lee R, Lubetkin E. I think therefore I am: perceived ideal weight as a determinant of health. Am J Public Health. 2008;98(3):501–506. Epub 2008 Jan 30.
14. Sarwer DB, Thompson JK, Cash TF. Body image and obesity in adulthood. Psychiatr Clin N Am. 2005; 28:69–87.
15. Currin L, Schmidt U, Treasure J, Jick H. Time trends in eating disorder incidence. Br J Psychiatry. 2005;186:132–135.
16. Christakis NA, Fowler JH. The spread of obesity in a large social network over 32 years. N Engl J Med. 2007;357(4):370–379. Epub 2007 Jul 25.
17. Mendes E. In U.S., self-reported weight up nearly 20 pounds since 1990. Gallup. November 23, 2011.
18. Kaiser State Health Facts. Adult Overweight/Obesity Rate by Gender. Kaiser State Health Facts, n.d. http://www.statehealthfacts.org/comparetable.jsp?ind=90&cat=2&sub=26&yr=138&typ=2. Accessed 12/08/2011
19. British Broadcasting Corporation (BBC) TV brings eating disorders to Fiji’. May 20, 1999, sec. Health. http://news.bbc.co.uk/2/hi/health/347637.stm. Accessed 12/08/2011
20. Lake A, and Townshend T. Obesogenic environments: exploring the built and food environments. J R Soc Promot Health. 2006;126(6):262-–267.
21. Wadden TA, Volger S, Sarwer DB, et al. A two-year randomized trial of obesity treatment in primary care practice. N Engl J Med. 2011;365(21):1969–1979. Epub 2011 Nov 14.
22. Bardia A, Holtan SG, Slezak JM, Thompson WG. Diagnosis of obesity by primary care physicians and impact on obesity management. Mayo Clin Proc. 2007;82(8):927–32.
23. Jeffery AN, Voss LD, Metcalf BS, et al. Parents’ awareness of overweight in themselves and their children: cross sectional study within a cohort (EarlyBird 21). BMJ. 2005;330(7481):23–24. Epub 2004 Nov 26.
Category: Medical Student Notebook, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}