Use of Bovine Pericardium in Complex Hernia Repair
The Hole in the Wall with Samuel Szomstein, MD, FACS
This Month’s Featured Expert:
by Moses K. Shieh, DO, FACOS
Dr. Shieh is a Bariatric Surgeon and Specialist in Complex Abdominal Wall Reconstruction, Medical Director of Bariatric Surgery for Lee Memorial Health System, Fort Myers, Florida
Funding: No funding was provided in the preparation of this article.
FInancial disclosures: Dr. Shieh is a consultant for Synovis Surgical Innovations, St. Paul, Minnesota.
Bariatric Times. 2011;8(8):14–16
A Message from Column Editor
Samuel Szomstein, MD, FACS
Welcome to the August issue of “The Hole in the Wall”. In this issue, Moses K. Shieh, DO, FACOS, Medical Director of Bariatric Surgery for Lee Memorial Health System, Fort Myers, Florida, presents two interesting cases regarding the use of bovine pericardium in complex ventral hernia repair. These clinical scenarios illustrate some of the advantages of the uses of biological materials for abdominal wall repair. Initially, nonabsorbable synthetic meshes were used as prostheses, but they often led to complications, particularly in complex repairs and contaminated fields. In recent years, biologic grafts of various types have been developed to be more biocompatible. Hernia repair with biologic mesh is a growing and increasingly studied field, with numerous novel applications. Different types of biologic products are available and vary based on the following: 1) the species of origin; 2) whether collagen crosslinking is present; and 3) the type of tissue harvested and how it is sterilized and processed to make it acellular. The origin and architecture may vary, but the common goal of the biological products is to provide a strong collagen scaffold into which new collagen can be deposited in an organized fashion.
I hope you enjoy the column and look forward to your feedback, questions and comments.
Dr. Szomstein is the Associate Director of the Bariatric Institute and Section of Minimally Invasive Surgery at the Cleveland Clinic in Weston, Florida, and Clinical Associate Professor of Surgery, Florida International University
—–
Repairing complex hernias in patients with severe obesity, diabetes, and exposed synthetic mesh can pose challenges for surgeons. Compromised circulation can make such patients more vulnerable to postoperative infection and limit their chances for full recovery without subsequent hernias.
Selecting an optimal biological graft for hernia repair may increase the chance of successful recovery. The selected graft should revascularize rapidly and eventually become indistinguishable from normal tissue. This can decrease the risk of postoperative infection and assist in preventing hernia recurrence.
Two successful cases of complex hernia repair with bovine pericardium (Veritas® Collagen Matrix, Synovis Surgical Innovations, St. Paul, Minnestoa) are presented here.
CASE #1
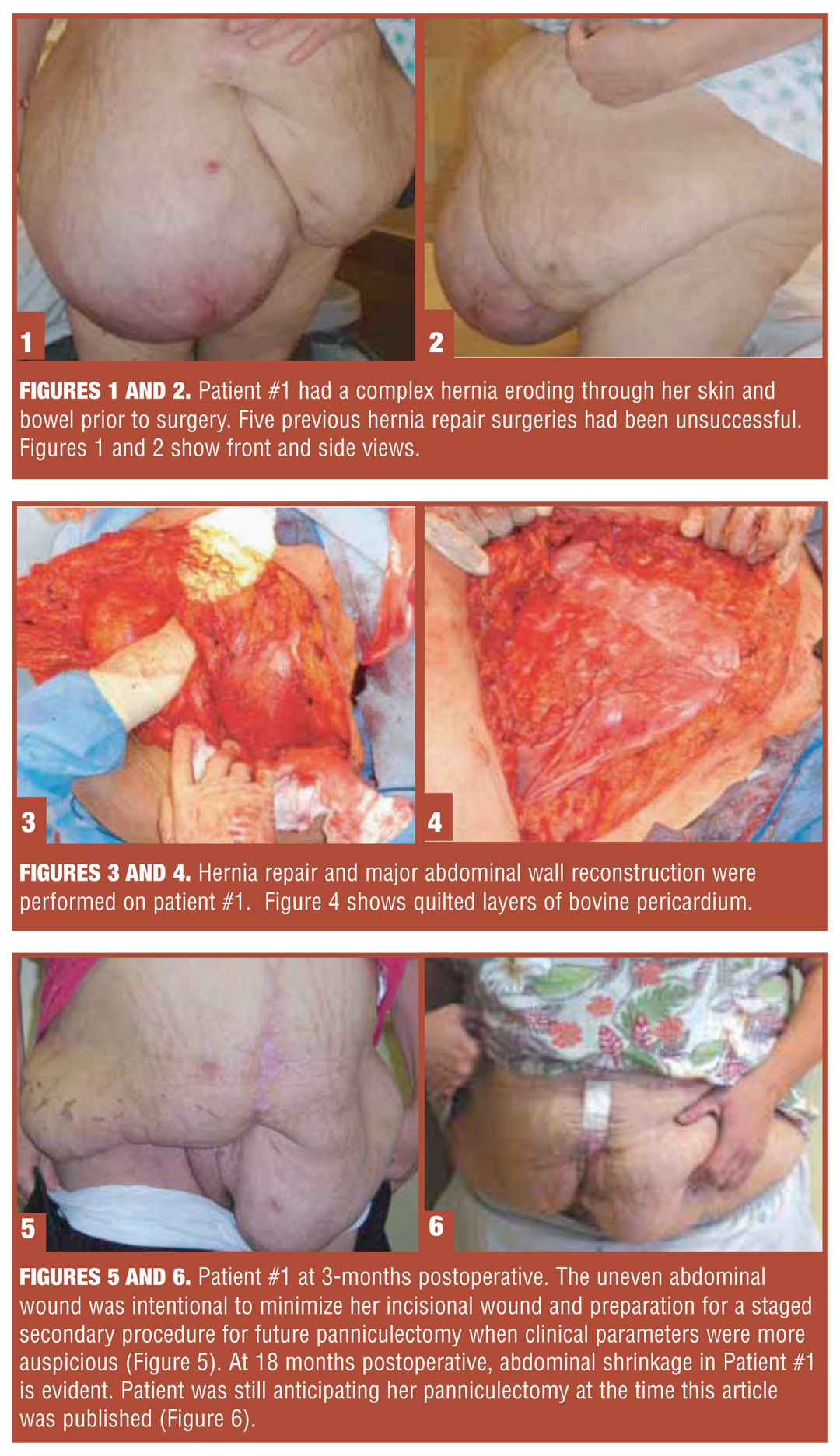
A 55-year-old, female patient, (height: 5’, weight: 260lbs) with a body mass index (BMI) of 50.8kg/m2, presented to the author’s facility in October 2008 with a severe abdominal wall hernia that was approximately the size of a basketball. The hernia was positioned outside of her peritoneal cavity and distended to her mid-thigh (Figures 1 and 2). Comorbid conditions included morbid obesity, diabetes, and chronic and active Methicillin-resistant Staphylococcus aureus (MRSA) wound infections on her abdominal skin wall. The patient had previously undergone five abdominal hernia repairs with synthetic mesh grafts. The surgeries were performed by different surgeons. All previous surgeries had had failed, potentially exacerbated by her obesity and type 2 diabetes mellitus (T2DM). The patient’s lower pannus was unable to support the weight of the repair from her previous surgeries, while her uncontrolled T2DM easily weakened previous repairs. At presentation, her hemoglobin A1C was 10.
The author (M. Shieh) made the decision to postpone surgery in order to optimize her blood sugar control and provide an opportunity for the superficial abdominal wounds to heal. She was referred to two different endocrinologists, who were unable to reduce her HgbA1C.
Three months later, the hernia defect had begun to erode through the patient’s skin. Bowel erosion through her abdominal skin wall was soon evident, and as a result, a major abdominal wall reconstruction was performed by the author (Figures 3 and 4). Three sheets of bovine pericardium (Veritas® Collagen Matrix, Synovis Surgical Innovations, St. Paul, Minnesota), each 12 x 25cm, were quilted together to provide a biological graft of the necessary size.
The patient proceeded through the usual clinical course. At one-month postoperative, dehiscence of the incision occurred. Wound cultures returned positive for MRSA despite treatment by two infectious disease teams. A computerized axial tomography (CAT) scan showed that the incision wound was also contaminated with MRSA, yet the hernia repair with bovine pericardium was intact. The infectious disease specialists advocated for removal of the bovine pericardium, considering it to be a foreign body; however, from a surgical perspective, it was believed that unless the patient’s hernia remained closed with the bovine pericardium, she would not recover. Since she was stable, the surgical recommendation prevailed and the bovine pericardium was kept in place. Continued incisional wound debridements were made to keep the wound clean. Once viable tissue was established, negative pressure wound therapy (V.A.C., Kinetic Concepts, Inc., San Antonio, Texas ) was applied.
During recovery (Figures 5 and 6), the patient was able to begin a protein-rich, low-fat, and low-carbohydrate diet and regular exercise routine. At 15 months postoperative, her hemoglobin A1C had decreased to 7. Her weight had decreased to 225 pounds (BMI: 44kg/m2) with an excess weight loss (EWL) of 26 percent. Repeated CAT scans have shown no recurrent hernia.
Case #2
In March 2008, a 49-year-old man fell 10 to 15 feet while at work. The fall resulted in a bowel injury and a ruptured spleen, which was immediately removed by a surgical trauma team. During his critical care stabilization and hospitalization, he was left with an open abdomen due to abdominal compartment syndrome.
Seven months later, the patient continued to maintain both an exposed abdomen and granulated tissue over his bowel. In addition, his anterior abdominal wall could not be brought back to midline due to excessive lateral contraction and persistent bowel edema. To address this, the trauma service proceeded with three surgeries using polytetrafluoroetylene (PTFE) mesh in hopes of closing his abdomen. Following the surgeries, a peripherally inserted central catheter (PICC) line was established and continuous dressing changes ensued. He subsequently developed MRSA in both his abdomen and the synthetic mesh graft.
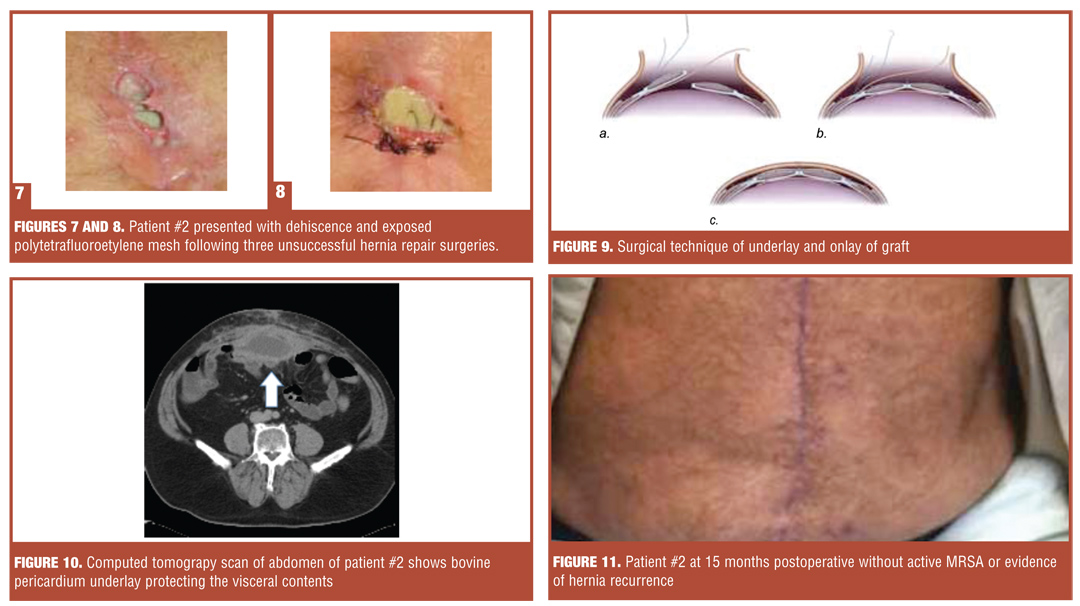
The patient presented to the author’s facility 18 months after his initial traumatic event for a complicated abdominal wall reconstruction. Preoperative photos showed dehiscence and the exposed graft (Figures 7 and 8).
The patient underwent surgery, during which the infected PTFE mesh (MRSA positive) was extracted and bovine pericardium was applied to close his abdomen in a single operation. A component separation as described by Ramirez et al[1] was performed using a unique sandwiched layer of two (12cm x 25cm) sheets of bovine pericardium. The first sheet (12cm x 25cm) was used as an underlay below the musculofascial layer with a 4 to 5cm overlap of the hernia defect to protect the peritoneum and its visceral contents. The second sheet (12cm x 25cm) of bovine pericardium was used as an overlay on top of the myofascial separation component. Sandwiched between these two layers was the injection of fibrin glue to minimize seroma formation as well as minimize migration of the grafts (Figure 9). The patient’s recovery in the hospital was uneventful, and he was discharged on postoperative Day 7.
Postoperative Day 30, with symptoms of abdominal pain, a CT scan demonstrated 3 to 4cm of fluid collection below the rectus abdominis muscle but above the underlay of bovine pericardium, which had been placed on top of the bowel (Figure 10). CT-guided aspiration of the seroma was positive for MRSA.
The infectious disease team recommended removing the bovine pericardium; however, since the patient was clinically stable, he was continued on long-term intravenous (IV) antibiotics and percutaneous drainage to treat the MRSA. Surveillance for signs and symptoms of an infected graft and/or recurrent hernia was conducted for several months.
At 15-months postoperative, the patient’s abdomen remained closed and showed no signs of recurrent hernia. In addition, there was no evidence of any active infection (Figure 11).
Discussion
Bovine pericardium offers surgeons an important option in repairing complex hernias in patients who have severe obesity, diabetes, and/or poor vascular bed perfusion/circulation. A commonly accepted premise of biologic grafts is their inherent ability to minimize infection and/or be placed in a contaminated wound.[2,3,4] Recent studies have shown that cross-linked biologic grafts may be more susceptible to bacterial colonization,[5] and it may not be prudent to place a cross-linked biologic graft within a contaminated surgical field as the chemical cross-linking process and subsequent lack of cellular infiltration may render the body incapable of clearing the infection.[6] In contrast, bovine pericardium (specifically Veritas, which was used in these patient cases) is non-cross linked. Non-cross-linking technology has been shown to facilitate earlier[7] host cell migration between graft and native tissue, providing a healthy source of host cell response to prevent or minimize infections better than other cross-linked biologic grafts.[8]
Case #1 and Case #2 illustrate three additional unique advantages of bovine pericardium application in complex abdominal wall repair: 1) quilting multiple sheets together offers a good option to provide adequate coverage of the abdominal wall defect;[3,9] 2) inherent biologic bovine pericardium enables excellent host cell infiltration, wound contraction, and wound healing as well as remodeling;[3,7] and 3) if bovine pericardium were to break down due to postoperative infection, a fibrotic reaction would occur, providing some reasonable support of scaffolding to provide abdominal wall support.[3]
The ability of non-cross linked bovine pericardium (specifically Veritas) to vascularize also helps to decrease the risk of infection.[4,7] This has always been a critical issue but is even more important in the era of outcome-based medicine. Recent Centers of Medicare and Medicaid Services (CMS) incentived to prevent surgical site infections[10] will soon result in third-party payers examining each surgeon’s outcomes. As these cases indicate, using non-cross linked bovine pericardium can improve patient outcomes while assisting surgeons in meeting this clinical requirement.
The unique bioengineered contouring gives non-cross linked bovine pericardium the most natural feel among all the biological grafts and makes it easy to handle. Non-cross-linked bovine pericardium does not require product-specific preparation or reconstitution with saline prior to use. This can improve intraoperative efficiency and reduce surgical time, thereby decreasing accumulation of inflammatory mediators and edema in the soft tissue of a patient with an exposed abdomen under anesthesia and can improve the quality of tissue approximation in closing the abdomen.[3]
Conclusion
Bovine pericardium offers the following important advantages over other biologic grafts: 1) it minimizes adhesions; 2) is pliable, yet strong; 3) is ready to use out of the package; 4) allows for easy suturing; and 5) remains consistent and uniform. Bovine pericardium has been used in hiatal hernia, vascular, carotid endarterectomy, and bariatric cases, as well as in staple line reinforcement, and can confidently and conveniently be used in laparoscopic as well as open surgery.
References
1. Ramirez OM, Ruas E, Dellon AL. Components separation method of closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 2003;112:106–14.
2. Wicker H. Management of abdominal wall defects in contaminated and dirty wounds. 2008. Synovis® Surgical Innovations.
3. Limpert JN, Desai AR, Kumpf AL, et al. Repair of abdominal wall defects with bovine pericardium. Am J Surg. 2009; 198(5):e60–655. Epub 2009 Oct 6
4. Ventral Hernia Working Group: Breuing K, Butler CE, Ferzoco S, et al. Incisional hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery. 2010;148(3):544–558. Epub 2010 Mar 20.
5. Gaertner WB, Bonsack ME, Delaney JP. Experimental evaluation of four biologic prostheses for ventral hernia repair. J Gastrointest Surg. 2007; 11(10):1275–1285.
Epub 2007 Aug 3
6. Alitizer A, Davidson J, Hiles M. Chemical cross-linking and biologic grafts. General Surgery News. 2010; 37(10):8–9.
7. Deeken CR, Melman L, Jenkins ED, et al. Histologic and biomechanical evaluation of crosslinked and non-crosslinked biologic meshes in a porcine model of ventral incisional hernia repair. J Am Coll Surg. 2011; 212(5):880–888. Epub 2011
Mar 23.
8. Harth KC, Broome AM, Jacobs MR, et al. Bacterial clearance of biologic grafts used in hernia repair: an experimental study. Surg Endosc. 2011;25(7):2224–2229. Epub 2011 Feb 7.
9. Mavrilas D, Sinouris EA, Vynios DH, Papageorgakopoulou N. Dynamic mechanical characteristics on intact and structurally modified bovine pericardial tissues. J Biomech. 2005;38(4):761–768.
10. Centers of Medicare and Medicaid Services (CMS) Surgical Care Improvement Project (SCIP). https://www.cms.gov/HospitalQualityInits/08_HospitalRHQDAPU.asp Accessed July 28, 2011.
Category: Hole in the Wall, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}