Ventral Hernias in Bariatric Surgery
The Hole in the Wall with Samuel Szomstein, MD, FACS
This Month’s Featured Experts
Mark D. Kligman, MD, FACS
Director Center for Weight Management and Wellness, University of Maryland School of Medicine, Baltimore, Maryland
Emanuele Lo Menzo, MD, PhD, FACS
Center for Weight Management and Wellness, University of Maryland School of Medicine, Baltimore, Maryland
Funding: No funding was provided in the preparation of this article.
FInancial disclosures: Drs. Kligman and Lo Menzo report no conflicts of interest relevant to the content of this article.
Bariatric Times. 2011;8(10):18–19
A Message from Column Editor
A Message from Column Editor
Samuel Szomstein, MD, FACS
Welcome to the October issue of “The Hole in the Wall.” This month, we are very honored to have Mark D. Kligman, MD, FACS, and Emanuele Lo Menzo, MD, PhD, FACS, from the Center for Weight Management and Wellness at the University of Maryland School of Medicine as our guest experts. They give us a great overview on and their insights about the controversial topic of Incidental hernias in bariatric surgery and their management options. Ventral/incisional hernias in bariatric surgery and their management is an ongoing debate and should be evaluated on the basis of patient safety and quality of outcomes. This requires good preoperative planning when possible and consideration of several options, such as multidisciplinary approach with other specialties like plastic/cosmetic surgery, staged operations, and the use of of special techniques and/or materials. Hernia treatments have become more complex, and therapeutic options have evolved, requiring better knowledge, skills, and equipment. We hope you will enjoy this column, and we look forward to your questions, comments and participation in future issues.
—–
Beside the well-known metabolic derangements, morbid obesity is responsible for an increased incidence of abdominal wall defects, both primary and secondary. Responsible for this association are chronically elevated intra-abdominal pressure, diabetes, steroid use, chronic obstructive pulmonary disease, and muscular atrophy.
It has been reported that at least eight percent of the patients undergoing bariatric surgery have known ventral hernias.1 This can potentially affect not only the choice of bariatric procedure, but also the technique utilized (e.g., trocar position, use of mesh).
The strict association between obesity and hernias and the wide-spread popularity of bariatric surgery will likely result in a more frequent discovery of ventral hernias during weight loss procedures. This is especially true since the preoperative physical exam is often unreliable.
Here, we offer a review of the available options to approach ventral hernias discovered either preoperatively or incidentally at the time of bariatric surgery.
Ventral hernia known prior to bariatric surgery
Whenever the diagnosis of hernia is made prior to the bariatric operation, several options are available. Although the ideal timing for hernia repair remains controversial, the following are a few scenarios:
1. Hernia repair prior to bariatric surgery
2. Surgical weight loss followed by hernia repair
3. Simultaneous bariatric procedure and hernia repair.
In general, unless the patient is symptomatic, repairing the hernia first is usually not recommended, and it might complicate future bariatric operations.[2] In fact, it has been previously reported that hernia repair in patients with obesity leads to longer hospital stay and higher complication and recurrence rates, even if performed laparoscopically.[3] The morbidity further increases when conversion to an open approach is necessary, as is often the case in patients with morbid obesity, because of larger hernia defects, increased likelihood of previous repairs, and technically challenging operations.
Bariatric surgery prior to hernia repair presents several advantages. The likely resolution of comorbid conditions, such as hypertension and diabetes, will result in decreased postoperative complications, both systemic and of the surgical site.[4] Also, the repair could be technically easier. The addition of panniculectomy at this stage can further improve results and patient satisfaction.[5]
The main drawback of a staged repair remains the potential for hernia-related complications (e.g., incarceration and strangulation), reported in 3.7 to 35 percent of cases.[5,6] This variability seems to correlate with the defect size (i.e., higher rates for smaller defects). For this reason, some authors advocate for concurrent repair of small defect during the bariatric operation and staged approach for the larger ones.[5]
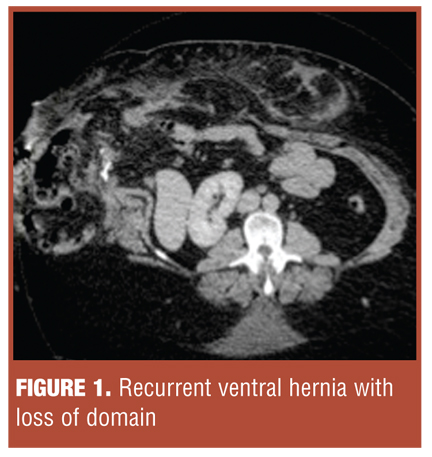
The choice of bariatric procedure must be considered carefully, and preoperative imaging studies might be necessary to assess its feasibility. In fact, extensive involvement of the small bowel in the hernia might limit the available working field (Figure 1).
Ventral hernia discovered during bariatric procedure
Management of ventral hernias discovered unexpectedly during bariatric surgery can pose a challenging dilemma. Options for management include the following:
1. Deferring definitive hernia repair;
2. Primary hernia repair
3. Prosthetic mesh repair
4. Biologic mesh repair.
The choice is largely dictated by several factors, including hernia size, presence of symptoms, type of bariatric procedure (clean vs. clean-contaminated), and the natural history of hernias.
Deferring definitive hernia repair. Definitive repair can be deferred with asymptomatic hernia, even if chronically incarcerated, as long as the hernia is left undisturbed during the bariatric procedure. However, vigilant followup is necessary[1] as the incidence of incarceration and strangulation increases during the weight loss process. Conversly, if the hernia must be reduced in order to complete the bariatric procedure, there is a high incidence of postoperative bowel obstruction (up to 35% in some series), which can lead to bowel ischemia, gastric remnant perforation, and gastrojejunostomy disruption.[6]
Primary hernia repair. Primary hernia repair has the advantages of technical simplicity and speed. However, the technique is only suitable for small defects (<3–4cm); primary repair of larger defects carries an unacceptably high recurrence rate—22 to 100 percent in bariatric series and up to 51 percent in larger hernia studies.[5–7]
Prosthetic mesh repair. Tension-free repair is the gold standard for larger hernias; however, the type of prosthesis to use remains controversial.[8] The use of synthetic prosthetics in clean-contaminated fields is associated with a significant risk of wound complications—seromas 25 percent and infection 33 percent.[4] Synthetic mesh infection can lead to additional operations for mesh removal and, ultimately, larger and more complex defects.
Biologic mesh repair. The advent of biologic mesh, extracellular matrix scaffolds derived from various sources, has revolutionized the approach to hernia repair in clean-contaminated and contaminated field. While these products vary on the basis of source (xenogenic or allogenic), tissue (pericardium, epidermidis, intestinal submucosa), and chemical alterations (cross-linked or not), they are resistant to infection, and thus, they can be utilized in clean-contaminated and contaminated fields (non-cross-linked products).
Unfortunately, biologic mesh is not an ideal solution. It is expensive and, additionally, early and mid-term recurrences, especially when used to bridge defects, have been reported.[10]
More recently, the use of synthetic mesh in clean cases (e.g., adjustable gastric band) to maximize the repair’s durability and biologic prosthetic in clean-contaminated cases (e.g., gastric bypass, sleeve gastrectomy) to minimize infectious complications, has been challenged. Several authors have reported the safety of synthetic nonabsorbable mesh (specifically light-weight, wide-pore mesh) in clean-contaminated cases.[4] This development demonstrates that the optimal approach to ventral hernia during bariatric surgery may change as new techniques and products are developed.
Conclusion
Currently, the lowest recurrence and complication rates will be achieved if the hernia repair can be deferred until the patient reaches a stable weight. If the hernia is discovered incidentally and can be left undisturbed, deferring the repair is feasible, but close followup is necessary.
If the hernia repair must be completed during the bariatric procedure, primary repair is appropriate for small defects, while mesh should be used in larger defects. Synthetic mesh is appropriate for clean cases and biologic mesh should be reserved for clean-contaminated cases. Despite some encouraging safety data, the use of prosthetic mesh in clean-contaminated cases remain controversial.
References
1. Datta T, Eid G, Nahmias N, Dallal RM. Management of ventral hernias during laparoscopic gastric bypass. Surg Obes Relat Dis. 2008;4(6):754–757.
2. Park A, Lo Menzo E. The surgeon’s lounge. Gen Surg News. 2010;37(3): 26–28.
3. Tsereteli Z, Pryor BA, Heniford BT, et al. Laparoscopic ventral hernia repair (LVHR) in morbidly obese patients. Hernia. 2008;12(3):233–238.
4. Rao RS, Gentileschi P, Kini SU. Management of ventral hernias in bariatric surgery. Surg Obes Relat Dis. 2001;7(1):110–116.
5. Newcomb WL, Polhill JL, Chen AY, et al. Staged hernia repair preceded by gastric bypass for the treatment of morbidly obese patients with complex ventral hernias. Hernia. 2008;12(5):465–469.
6. Eid GM, Mattar SG, Hamad G, et al. Repair of ventral hernias in morbidly obese patients undergoing laparoscopic gastric bypass should not be deferred. Surg Endosc. 2004;18(2):207–210.
7. Hesselink VJ, Luijendijk RW, de Wilt JH, Heide R, Jeekel J. An evaluation of risk factors in incisional hernia recurrence. Surg Gynecol Obstet. 1993;176(3):228–234.
8. Herbert GS, Tausch TJ, Carter PL. Prophylactic mesh to prevent incisional hernia: a note of caution. Am J Surg. 2009;197(5):595–598; discussion 598.
9. Breuing K, Butler CE, Ferzoco S, et al. Incisional ventral hernias: review of the literature and recommendations regarding the grading and technique of repair. Surgery. 2010;148(3):544–558.
10. Jin J, Rosen MJ, Blatnik J, et al. Use of acellular dermal matrix for complicated ventral hernia repair: does technique affect outcomes? J Am Coll Surg. 2007;205(5):654–660.
Category: Hole in the Wall, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}