
Myths Associated with Obesity and Bariatric Surgery—Myth 2: “Bariatric surgery induces weight loss primarily by mechanical restriction and nutrient malabsorption.”
May 2012
Exclusive Series: The Metabolic Applied Research Strategy Initiative
Bariatric Surgery: Beyond Restriction and Malabsorption
Myth 2: “Bariatric surgery induces weight loss primarily by mechanical restriction and nutrient malabsorption.”
by Lee M. Kaplan, MD, PhD; Randy J. Seeley, PhD; and Jason L. Harris, PhD
Bariatric Times. 2012;9(5):12–13
Abstract
The Metabolic Applied Research Strategy is a multi-year, multi-generational collaborative research program between the Massachusetts General Hospital, the University of Cincinnati, and Ethicon Endo-Surgery. Its focus is to interrogate and understand the physiologic and metabolic changes that occur after bariatric surgery (i.e., how bariatric surgery works to resolve conditions such as type 2 diabetes) with the goal of inventing new, less invasive, and less expensive treatments for patients suffering from obesity and its related health issues. In this article, which is the third in a series of articles published in Bariatric Times dedicated to the Metabolic Applied Research Strategy initiative, the authors discuss past and present understanding on why bariatric surgery works, its true mechanisms of action, and how these findings might help researchers, surgeons, and industry harness the remarkable effectiveness of bariatric surgery.
LEE M. KAPLAN, MD, PhD
Lee M. Kaplan, MD, PhD, is Director of the Obesity, Metabolism & Nutrition Institute at Massachusetts General Hospital (MGH) and Associate Professor of Medicine at Harvard Medical School. He is the Director of the subspecialty Fellowship Program in Obesity Medicine and Nutrition at MGH; Associate Director of the NIH-sponsored Boston-area Obesity and Nutrition Research Center; a member of the NIH Clinical Obesity Research Panel; and past chairman of the Board of the Campaign to End Obesity. Dr. Kaplan’s clinical expertise is in the areas of obesity medicine, gastroenterology, and liver disease. His research program is focused on understanding the mechanisms by which the gastrointestinal tract regulates metabolic function and using physiological and genetic approaches to identify therapeutically relevant subtypes of obesity and its complications.
RANDY J. SEELEY, PhD
Dr. Randy J. Seeley is Professor of Medicine and holds the Donald C. Harrison Endowed Chair at the University of Cincinnati College of Medicine. In 2009, Dr. Seeley was appointed as the Director of the Cincinnati Diabetes and Obesity Center (CDOC). His scientific work has focused on the actions of various peripheral hormones in the central nervous system that serve to regulate food intake, body weight, and the regulation of circulating fuels. In particular, he focuses upon the numerous hypothalamic and gastrointestinal peptides and their associated receptors that influence both energy intake as well as peripheral metabolic processes with the aim of developing new treatment strategies for both obesity and diabetes.
JASON L. HARRIS, PhD
Dr. Jason L. Harris is a Principal Engineer leading Metabolic Applied Research Strategy co-invention and product development efforts at Ethicon Endo-Surgery, a Johnson and Johnson company. Since 2006, he has been exploring novel treatment approaches for patients suffering from the effects of metabolic disease. His primary focus is applying insights from basic and applied research efforts to develop improved therapies and predictive tools for the treatment of this disease.
———
Introduction
Beginning in the 1950s, several thoughtful and creative surgeons developed a variety of procedures to promote weight loss and combat obesity. Based on the then-current understanding of the causes of obesity, the goals of these surgical procedures were to restrict the patient’s ability to overeat and/or to prevent absorption of the ingested calories. Over the past several decades, with the development of new procedures, technical advances, increased surgical experience, and improved pre-, peri- and post-operative care, the overall safety and effectiveness profiles of bariatric procedures have improved substantially. Today, bariatric surgery remains the most effective long-term treatment of obesity by a wide margin. Moreover, bariatric procedures have been shown to strongly enhance the management of diabetes and other metabolic disorders in ways that can complement or substitute for currently available medical therapies.
Reconsidering Mechanisms of Action
The uniquely high efficacy of these procedures begs the question of how they work. Although initially developed as a means of promoting food restriction and/or macronutrient malabsorption, a variety of clues suggests that these operations work by other means.
Restriction. It seems surprising that restriction of food intake at the level of the proximal stomach would be effective when restricting food by physically wiring a patient’s jaw shut has been so ineffective. Indeed, after jaw wiring, patients remain hungry and seek means of bypassing the mechanical restriction.[1] In contrast, after gastric “restriction” procedures, most patients describe a decrease in hunger and other appetitive drives, suggesting that these operations influence central nervous system (CNS) pathways that regulate food intake.
Malabsorption. Operations that are demonstrably malabsorptive of macronutrients, such as the jejunoileal bypass and biliopancreatic diversion (BPD), have been shown to be associated with decreased food intake in both human patients and animal models. In contrast, diseases and operations that generate isolated protein-calorie malabsorption are typically associated with an increase in hunger and food intake as a means of trying to counteract the missing calories. The decreased hunger associated with “malabsorptive” bariatric procedures suggests that these operations primarily modulate CNS regulation of appetite.
Physiological changes. Beyond the dramatic changes in hunger, satiety, and reward-based appetitive drives, several additional clinical observations support a primarily physiological mechanism of weight loss after bariatric surgery. Few patients become underweight after surgery unless a complication ensues. It would be common to expect such “overshooting” if the mechanisms were primarily mechanical. In addition, patients who become pregnant after bariatric surgery typically gain weight appropriately, suggesting that the physiological changes during pregnancy can overcome even the powerful physiological effects of bariatric surgery. Bariatric surgery occasionally performed on relatively thin patients (BMI<30kg/m2) or animal models is associated with minimal weight loss. Moreover, several gastrointestinal (GI) peptide hormones that regulate appetite, including ghrelin, glucagon-like peptide-1 (GLP-1), peptide YY (PYY), CCK, and amylin, change after diversionary (bypass) bariatric procedures and sleeve gastrectomy in ways that are the opposite of changes induced by voluntary or forced dietary restriction.[2,3] While not necessarily the primary cause of the associated weight loss, the changes in the circulating concentrations of these hormones after surgery suggest that they contribute to a changed postoperative physiology. In contrast, the opposite changes observed after dietary restriction suggest the body’s attempt at physiological counter-regulation to combat the induced weight loss.[4] The absence of this counter-regulatory effect after surgery clearly demonstrates that food restriction is not the primary mechanism of action, at least for the various diversionary procedures and sleeve gastrectomy. Finally, recent studies have demonstrated that isolated genetic manipulation can block the weight loss effects of Roux-en-Y gastric bypass (RYGB), a dramatic outcome that would not be expected to occur if the surgery worked primarily through mechanical (restrictive or malabsorptive) mechanisms.
The Physiological Model
Numerous recent studies in human patients and animal models have provided strong evidence for the physiological model of bariatric surgery. Together, they demonstrate that these effects are fundamentally and broadly different from the effects of weight loss by other means, such as dietary restriction. As described in Part 2 in this series,[5] under normal circumstances, body weight is tightly regulated by a complex network that controls energy balance and metabolic function. A major output of this powerful network is the defense of an appropriate physiological set point for body fat mass. Obesity results from one or more disruptions in this network that lead to defense of an abnormally high set point, and the current epidemic of obesity likely results from the effects of changes in our modern environment on this regulatory network. A major environmental contributor appears to be the progressive change in the chemical composition of the food supply, with an abundance of homogeneous and processed foods, which both incorporate non-natural additives (e.g., preservatives, trace concentrations of hormones and antibiotics) and lack many substances (e.g., fiber, phytochemicals, and other trace compounds) normally present in natural foods. These ingested foods likely alter the normal signaling from the gut to the brain and elsewhere, thereby affecting the normal physiological regulation of energy balance and metabolic function (Figure 1). By altering signals emanating from the GI tract, bariatric surgery appears to counteract these environmental effects. Ultimately, surgery causes changes in the regulatory network so as to reset the physiological set point for fat mass to a level closer to normal.
So how does bariatric surgery cause these changes? And why are the effects so profound and durable? Answering these questions and harnessing the resulting understanding to develop effective but less invasive therapies are the primary goals of the Metabolic Applied Research Strategy (MARS) and similar research efforts.
Specific Physiological Mechanisms
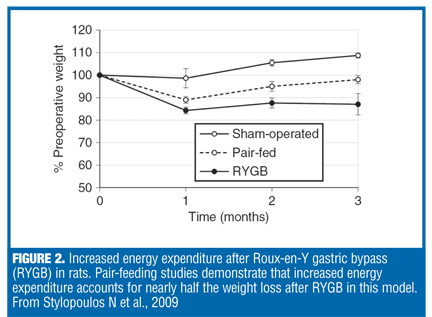
Changes in appetitive drives and energy expenditure. Numerous human studies and preclinical studies in animal models have demonstrated that several bariatric procedures cause patients to experience changes in food preference, increased satiety, decreased hunger and reward-based eating, improvements in glucose metabolism out of proportion to the induced weight loss and blunting of the metabolic adaptation (decreased energy expenditure) that normally accompanies weight loss. Dramatically in rodent models and to a lesser extent in human patients, diversionary procedures, such as RYGB and BPD, induce an increase in resting and diet-induced energy expenditure, an effect that contributes substantially to the associated weight loss.[6] In diet-induced obese rats, only about half of the weight loss after RYGB can be attributed to the reduction in food intake associated with the procedure (Figure 2), with increased energy expenditure accounting for the rest (there is a negligible contribution from increased caloric excretion in the stool).
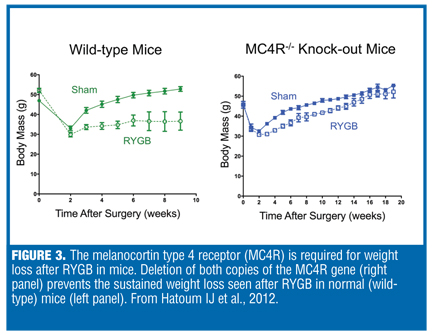
MC4R gene. The pathways underlying the stimulation of energy expenditure after RYGB remain largely unknown. Neuronal signaling through the melanocortin type 4 receptor (MC4R) is known to be a critical regulator of energy expenditure, so we hypothesized that the MC4R signaling system might be required for the effects of RYGB. A recent study by Hatoum et al[7] showed that genetic deletion of the MC4R gene blocks the ability of RYGB to induce weight loss and reduce body fat mass in mice (Figure 3). Interestingly, only animals with deletions of both copies of the gene MC4R were resistant to the normal outcomes of surgery. Those with one mutated and one normal copy of the gene responded normally to RYGB, which explains why human patients with MC4R mutations (nearly all of whom have only one mutated copy) respond normally to this operation.
Gut hormones. Recognizing the powerful physiological effects of RYGB and other bariatric surgical procedures, we still do not know precisely how structural alterations in the GI tract influence this physiology. As noted previously, the levels of several gut regulatory peptides change in a manner that could contribute to decreased food intake and improved glucose homeostasis. Proving their contribution is more difficult, but studies using a pharmacological inhibitor (exendin-9) have provided strong evidence that increased postprandial GLP-1 levels after surgery contribute to the improvement in insulin secretion, if not insulin sensitivity or weight loss.8 One study using antibodies to PYY suggests an important role of this peptide as well.
Other changes. Beyond altered gut hormone levels, bariatric surgery induces changes in the levels, distribution, or activity of a variety of other factors known to regulate energy balance and metabolic function. These include altered vagal and sympathetic neural activity, increased circulating bile acids, changes in the distribution of bacteria in the gut microbiota, and many others. The relative importance of changes in these different systems is currently unknown, but the dramatic changes in each of them provide further support for the physiological basis of these operations.
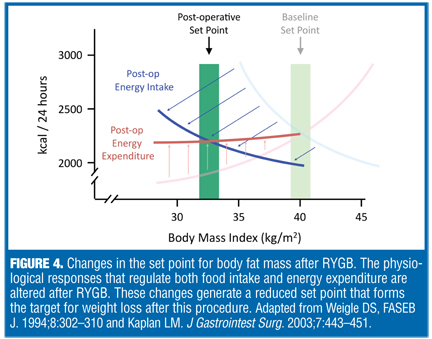
Postoperative set point. Within the framework of a physiological set point, and based upon growing evidence in the literature, we may view bariatric surgery as driving the defended set point to a lower level, leading to decreased fat mass and body weight (Figure 4). The new set point is defended similarly to the inappropriately high preoperative set point. As a result, dietary restriction to augment surgically-induced weight loss is likely to be as difficult and unsuccessful as similar attempts occurring before the operation. However, the postoperative set point remains susceptible to additional physiological influences, thus explaining the retained response to pregnancy after surgery and the continued susceptibility to the broadly obesogenic environment that can promote late postoperative weight regain.
Discussion
Despite the profound positive impact bariatric surgery has on patient health, the percentage of eligible patients who undergo these operations remains very low. There are several likely reasons for this limited utilization, including misconceptions about the causes of obesity and the effectiveness of nonsurgical therapies, the perceived appropriateness of a surgical solution, and the overall risk-benefit profile of surgery. To the degree that we misconstrue obesity as either a primarily voluntary or behavioral problem (rather than a primarily physiological disorder), we are likely to reject surgery as an inappropriate solution. Such conclusions are reinforced by overestimation of the benefit of lifestyle or pharmacological interventions. They are further reinforced by misapprehension of the true risks, benefits, and costs of each of the various bariatric procedures. Fortunately, several recent studies, including three well-controlled and well-publicized clinical trials, provide a more accurate picture to patients and the general medical community.[9–11] Nonetheless, the concept that surgery acts primarily through behavioral modification, by forcing diminished food intake or malabsorption of ingested calories, can promote a sense of mismatch between the severity of the disease and the invasiveness of the treatment.
Fortunately, we now know that forced behavioral change is not the dominant outcome. Through mechanisms that are not completely understood, surgery alters the endogenous regulators of body weight, body fat, and metabolic function. Bariatric surgery can thus be considered as a particularly powerful type of medical therapy, a “pharmacology on steroids,” that should make it more understandable, and thus more acceptable, to those of us who need, support, and pay for its use.
References
1. Elder KA, Wolfe BA. Bariatric surgery: a review of procedures and outcomes. Gastroenterology. 2007; 1232:2253–2271.
2. Le Roux CW, Aylwin SJ, Batterham RL, et al. Gut hormone profiles following bariatric surgery favor an anorectic state, facilitate weight loss, and improve metabolic parameters. Ann Surg. 2006;243:108–114.
3. Korner J, Bessler M, Cirilo LJ, et al. Effects of Roux-en-Y gastric bypass surgery on fasting and postprandial concentrations of plasma ghrelin, peptide YY and insulin. J Clin Endocrinol Metab. 2005;90:359–365.
4. Sumithran P, Prendergast LA, Delbridge E, et al. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365:1597–1604.
5. Kaplan LM, Seeley RJ, Harris J. Myths associated with obesity and bariatric surgery: Myth 1: Weight can be reliably controlled by voluntarily adjusting energy balance through diet and exercise. Bariatric Times. 2012;9(5)12–13.
6. Stylopoulos N, Hoppin AG, Kaplan LM. Roux-en-Y gastric bypass enhances energy expenditure and extends lifespan in diet-induced obese rats. Obesity. 2009;17:1839–1847.
7. Hatoum IJ, Stylopoulos N, Vanhoose AM, et al. Melanocortin-4 receptor signaling is required for weight loss after gastric bypass surgery. J Clin Endocrinol Metab. 2012 Apr 6. [Epub ahead of print]
8. Salehi M, Prigeon RL, D’Alessio DA. Gastric bypass surgery enhances glucagon-like peptide 1-stimulated postprandial insulin secretion in humans. Diabetes. 2011;60(9):2308–2314.
9. Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012; 366:1567–1576.
10. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012;366:1577–1585.
11. Leonetti F, Capoccia D, Coccia F, et al. Obesity, type 2 diabetes mellitus, and other comorbidities: a prospective cohort study of laparoscopic sleeve gastrectomy vs. medical treatment. Arch Surg. 2012 Apr 16. [Epub ahead of print]
FUNDING: No funding was provided.
DISCLOSURES: Dr. Kaplan has received research support from the National Institute of Diabetes and Digestive and Kidney Diseases (NIH), Ethicon Endo-Surgery, Merck Research Laboratories, and GI Dynamics. He has done consulting for C.R. Bard, Gelesis, Rhythm Pharmaceuticals, Medtronic, Sanofi-Aventis, Amylin Pharmaceuticals, Allergan, Merck, GI Dynamics, and Johnson & Johnson. Dr. Seeley has received research support, has done speaking or consulting for the following companies: Amylin Pharmaceuticals, Eli Lilly, Johnson & Johnson, Novo Nordisk, Zafgen Inc., Merck, Roche, Alkermes, and Pfizer. Dr. Harris is an employee of Ethicon Endo-Surgery.
Category: MARS Initiative Series, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}