
ASMBS News and Update—April 2012
by Robin L. Blackstone, MD, FACS, FASMBS
Dr. Blackstone is President of the American Society for Metabolic and Bariatric Surgery and Medical Director, Scottsdale Healthcare Bariatric Center, Scottsdale, Arizona.
ASMBS Mission Statement
The American Society for Metabolic and Bariatric Surgery was founded in 1983 to establish educational and support programs for surgeons and integrated health professionals. Our mission is to improve the care and treatment of people with obesity and related disease; to advance the science and understanding of metabolic surgery; to advocate for health care policy that ensures patient access to high-quality prevention and treatment of obesity. For more information, visit www. ASMBS.org. If you are interested in becoming a member or have questions about ASMBS, please contact Georgeann Mallory, the ASMBS Executive Director, via phone: (352)-331-4900 or e-mail: info@asmbs.org.
Metabolic and Bariatric Surgery (MBS) in 2012—Surgery is Proven Superior to Medical Therapy for Patients with Type 2 Diabetes
Robin Blackstone, MD; Bruce Wolfe, MD; and Jaime Ponce, MD
Over the last few weeks, two landmark papers[1,2] were published in the New England Journal of Medicine presenting randomized, prospective data against a medical comparator group in patients with type 2 diabetes mellitus (T2DM) and obesity in various clinical states. This represents the strongest data in our field proving the effect of surgery in treating diabetes in patients with body mass indices (BMIs) of 27kg/m2 and greater.
Friedman et al made the original observation that surgery affected T2DM in “The amelioration of diabetes mellitus following subtotal gastrectomy,” published in Surgery, Gynecology, and Obstetrics in February 1955.[3] Thirty-two years later in 1987, Pories et al[4] published the landmark observational study documenting the remission of T2DM in a large number of patients following Roux-en-Y gastric bypass (RYGB). Although our critics are already sounding notes of caution about the early follow up (two years) of the newly reported results, this work represents the tipping point for our specialty in regards to disease-specific treatment with metabolic surgery.
I propose that in light of this historic moment our specialty truly adopt Metabolic and Bariatric Surgery (MBS) as the official “content” of our work and use MBS in all communications regarding this specialty.
This confirms the decision to change the name of our society a few years ago and correlates well with the name of our unified quality program with the American College of Surgeons (ACS)—the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBS AQIP).
The National Institutes of Health (NIH) Consensus Statement on Gastrointestinal Surgery for Severe Obesity (consensus.nih.gov/1991/1991gisurgeryobesity084html.htm) as written in 1993 were defined for the treatment of obesity. Now, we are entering a different era of MBS where the primary treatment target is disease specific (e.g., treating diabetes) rather than obesity alone. This fundamental shift in the paradigm of treatment is crucial as it avoids the difficult perception that MBS is a cosmetic treatment rather than fundamental to the patient’s health and survival. It also avoids the difficult argument of personal responsibility in the development of the disease of obesity and the role of environment versus biology. These randomized, prospective data published in the NEJM suggest that MBS surgeons should be expanding surgical therapy to patients with T2DM, even in BMI groups less than 35kg/m2. We are finally free of arbitrary guidelines based on BMI.
Metabolic surgery is defined as those procedures that have either weight-independent effect of treatment, a weight-dependent treatment effect, or both. Examples of procedures that are both weight independent and dependent but primarily work through weight-independent effects include sleeve gastrectomy (SG), gastric bypass (RYGB), biliopancreatic diversion (BPD), and duodenal switch (DS). Adjustable gastric banding (AGB) is an example of a weight-dependent procedure as weight loss is its primary mechanism of action.
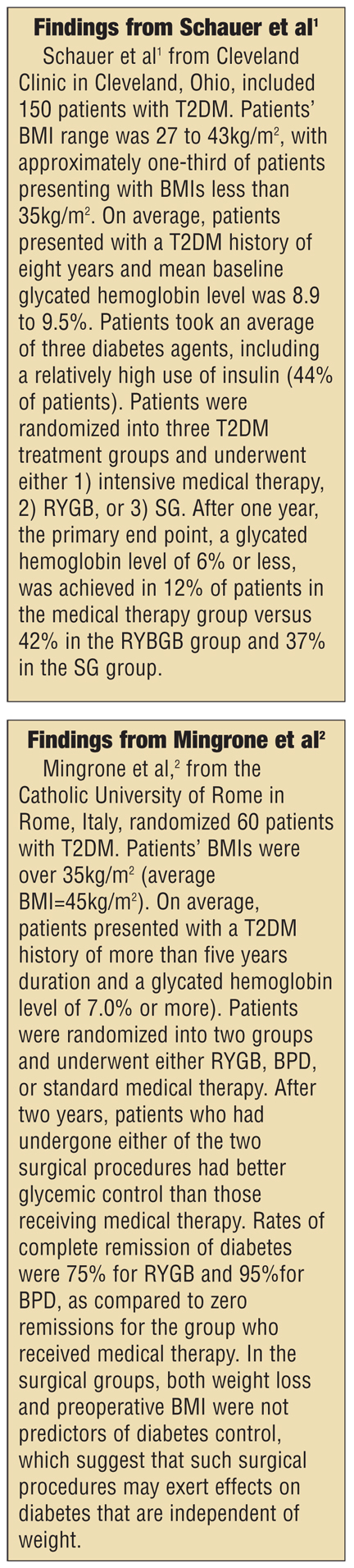
Dr. Ponce has summarized the two studies[1,2] recently published in NEJM (see sidebars “Findings from Schauer et al” and “Findings from Mingrone et al”).
Major findings and limitations summarized by Dr. Bruce Wolfe.
• The two studies1,2 demonstrating superior diabetes control and induction of remission among people with overweight, obesity, and severe obesity confirm using the most rigorous clinical research method available—observational research, which previously reported remarkable induction of T2DM remission following MBS. The prior research findings are thereby strengthened and given credibility.
• The durability of the effect of MBS on diabetes over a period of many years remains to be demonstrated. In any case, however, the development of devastating secondary complications of diabetes (vascular disease, neuropathy, blindness, kidney failure) can be expected to be delayed if not prevented altogether—an important contribution to health.
These two studies are likely to have a major effect on future diabetes treatment. Bariatric surgery should be included in future algorithms for the treatment of T2DM as suggested by the 2011 International Diabetes Federation (IDF) position statement.[5] Until now, only one randomized, controlled trial has shown the superiority of surgery (gastric banding) over medical care.[6] In that trial, patients with very early diabetes (diagnosis less than two years and only on metformin) were studied.
Remaining questions to be addressed by further research and the issue of durability of the effect
• How many patients with T2DM treated with medications, diet, and exercise can achieve a similar response to the response achieved by surgery? Can that number be increased in the future?
• Will surgery provide superior control of diabetes with secondary reduction of diabetes complications, as indicated by these studies, in most people with diabetes?
• To what extent will the long-term outcomes of T2DM be improved by surgery in comparison to continued medical treatment without surgery?
What should you do with this data and these findings?
These randomized, prospective studies with medical comparator groups finally provide data needed for acceptance by the payors and medical community in general. Surgeons and integrated health teams working in MBS should share the information contained in these studies. Armed with the knowledge of these studies, the call to action should be for our medical colleagues to include the option for surgery in their discussion with patients about the management of their T2DM.
Although the numbers of patients were limited in the STAMPEDE trial, patients with BMI below 35kg/m2 showed improvement when the diabetes control was not optimal by medical therapy.
Patients need to realize and understand that there is a surgical option that may limit the damage of long-term diabetes and simultaneously resolve many other medical conditions related through the common pathway of the inflammation of obesity.
We encourage you to integrate this knowledge into your public seminars, educational sessions, and continuing medical education (CME) events with patients and medical colleagues. To download a Powerpoint that can be used to communicate with your colleagues go to http://bit.ly/MetaSurg-T2Diabetes.
We also encourage you to attend the Metabolic and Bariatric Surgery Course at the upcoming ASMBS annual meeting where the most up to date understanding of this topic will be presented (course content listed in the following section).
Begin to think about the implications of advocating for the treatment of diseases specific to obesity rather than the obesity itself.
ASMBS Annual Meeting Course Schedule, June 17–20, 2012, San Diego, California
• Obesity and Cancer, Cancer, and Cancer Recurrence
A specific course on the relationship of cancer and cancer recurrence to obesity
Date: Thursday, June 21, 2012
Time: 3:45–5pm
• Mechanisms of Obesity and Bariatric Surgery
Date: Monday, June 18, 2012
Time: 8:00am–12:00pm
Course directors: Robin Blackstone, MD, Francesco Rubino, MD
Accreditation: Up to 3.75 CME credits available. Up to 4.0 CEU credits available.
Course overview and target audience: Bariatric researchers, bariatric surgeons, residents, fellows, and allied health members interested in pathophysiology of obesity and mechanisms of action of bariatric operations.
Course objectives: Upon completion of this session, participants will be able to do the following:
• Review biology of obesity related to energy and nutrient sensing, gut-brain signaling related to hunger and satiety, and glucose metabolism
• Recognize the pathophysiology of obesity related to inflammation, cancer risk, and the relationship between insulin resistance and obesity-related comorbidities
• Identify weight-loss independent effects of metabolic operations, changes in energy regulation and food choices after bariatric surgery, and mechanisms of improved glucose homeostasis.
Maintenance of certification: For bariatric researchers, bariatric surgeons, residents, fellows, and allied health members. This event will provide CME in their specific specialty to comply with Maintenance of Certification (MOC) in the following areas: 1) Medical knowledge, 2) Patient care, 3) communication skills, and 4) practice-based learning and improvement.
Course Outline
Session I: The Biology of Obesity
• 7:30am—Metabolic Programming by Joy Bunt, MD, PhD
• 7:50am—Role of the Gut in Obesity: The Mechanisms That Govern Hunger, Satiety and Glucose Metabolism (Gut Hormones, Bile Acid Exposure, and Microbiota) by Randy Seeley, PhD
• 8:10am—Body Weight Regulation: Not Just a Matter of Energy In and Energy Out by Lee Kaplan, MD, PhD
• 8:30am—Can You be Heavy and Healthy or Fat but Lean? Why Weight Metrics Do Not Predict Disease. Presenter TBD.
• 8:50am—Inflammation and Obesity by Robert O’Rourke, MD
• 9:10am—Cancer and Obesity by Ted Adams, PhD
• 9:40am—Panel discussion/Q and A
• 10:00am—Refreshment Break
Session II: The Mechanisms of Action of Surgery
• 10:15am—The Effect of GI Surgery vs. Non-surgical Weight Loss Interventions on Energy Expenditure by Lee Kaplan, MD, PhD
• 10:35am—The Metabolic Operations: Sleeve, GBP and DS by Ricardo Cohen, MD
• 10:55am—Weight-Independent and Weight-Dependent Mechanisms of Comorbidity Resolution by David Cummings, MD, PhD
• 11:15am—Gastric vs. Intestinal Mechanisms: Distinct Impact on Body Weight and Glucose Homeostasis by Francesco Rubino, MD
• 11:35am—Revision of Primary Bariatric Surgery through the Prism of Metabolic Mechanisms of Action by Robin Blackstone, MD
• 11:55am—Impact of Metabolic Surgery on the Brain: Cognition/Depression and Suicide by John Morton, MD
• 11:55am—Panel discussion/Q and A
• 12:15pm—Adjourn
Collecting and Using Data: Beyond the First Data Registry
by Robin Blackstone, MD
On April 1, 2012, the 458 accredited and 200 provisional programs of the ASMBS BSCOE program joined the programs in the ACS BSCN to form the Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program (MBS AQIP). Part of the process of integration is for the former ASMBS BSCOE programs to begin reporting to the ACS BSCN data registry. This data registry is a second-generation database streamlined and enhanced over the last few years. There are a number of new features that will be unfamiliar to the ASMBS Bariatric Centers of Excellence (BSCOE) programs and may cause some angst, but eventually programs will come to realize the many advantages of being in this second-generation environment. Let’s take a step back and examine why we enter data, the limitations of the previous database for the ASMBS programs, the Bariatric Outcomes Longitudinal Database (BOLD), and the opportunities to collect more accurate data that can be used at the local, state, and regional level for quality improvement.
It is clear that the future of all surgeons includes monitoring their outcomes through an established data registries. The American Board of Surgery (ABS) requires that all surgeons enter patients and adverse outcomes into a data registry to maintain certification. ABS MOC Part 4 requires ongoing participation in a national, regional, or local outcomes database or quality assessment program. Entry of data into the joint registry is also a requirement for accreditation of the MBS AQIP into which all previous ASMBS BSCOE and ACS BSCN programs belong as of April 1, 2012. Although these two purposes, certification and accreditation, are significant to our ability to practice our art, the most important reason to collect and monitor our own data is to improve the safety of surgery for our patients. In this goal we each need to take responsibility to assure that the collection of data is accurate and timely. This data will inform the national/regional-and state-based collaboratives being organized this year that will enable groups of MBS surgeons to work together to improve care.
Through our initial efforts at data collection with the BOLD registry, ASMBS BSCOE program members have learned a great deal that can be useful to us as we become part of the new data registry at the ACS. It is important to remember that first-generation registries always have significant opportunities for improvement. I offer the following considerations and limitations in previous data-entry processes and procedures, and information on how these will be addressed in the new data registry as a way of focusing our efforts moving forward into the new database.
Institutional review board issues. According to 45 CFR (Code of Federal Regulations) Part 164.501, 506, the use of patient data for quality improvement purposes is considered part of healthcare operations under the Health Insurance Portability and Accountability Act (HIPAA) and does not require review by an institutional review board (IRB). The attorneys for the ACS have also issued the following statement: “The ACS BSCN database is focused on capturing and analyzing data to determine overall quality measures and to ensure a participant’s compliance with the accreditation standards. The database is not part of a specific clinical study. Therefore, IRB approval is not necessary for participation.”
Eventually, participants in the MBS AQIP may wish to request aggregate outcomes data for research purposes. To accommodate these requests, a limited data set will be created periodically by the database vendor and provided to the ASMBS Research Committee for distribution to qualified investigators through a data use agreement. The database is managed by Outcome Sciences (Cambridge, Massachusetts), an independent contractor that is not a healthcare provider or insurance plan and will not be involved in the conduct of research using the database. Because the individuals conducting research will use only limited aggregate data and will not come in contact with the registry data-containing protected health information (PHI), IRB review of this activity will not be required.
Potential for bias in data entry. Previously entered data were self-reported by BSCOE participants in BOLD. Designated individuals entered into BOLD from each bariatric program. Some individuals conducting data entry are involved in patient care, including nurse practitioners/physician assistants providing direct patient care and surgeons. In the new database, a person who is not a provider of care, defined as surgeon or nurse practitioner, must do the data entry. The data entry by definition will be more independent and based on comparison of the clinical chart to strict definitions for adverse events. The overall quality of the data will improve and this source of bias eliminated.
Heterogeneity of data-entry personnel. There have never been specific qualifications required for individuals entering data into BOLD. Each surgical practice determined who within their program was most available to enter data and was responsible for their participation in the available BOLD training opportunities. The burden of paying for the data entry was placed on the surgeon even though the margins of profitability of the practice are far less than the facility. The assignment of BOLD data-entry responsibility varied across bariatric programs. For some programs, BOLD data entry was managed entirely by the surgical practice while for others it was shared between the practice and the hospital. While this practice accommodates a variety of program structures, it can potentially lead to variations in data-entry practices that can affect data quality.
The new data registry requires that each program identify a single data collector at its site. In addition, the data collector cannot be a surgeon or other personnel involved in patient care. It is recommended that preference be given to medically trained personnel and/or experienced chart abstractors. For most programs this obligation (and associated expense) will fall on the facility, which often already have experienced abstractor/quality personnel. The Bariatric Surgery Clinical Reviewer (person responsible for data collection) must be certified in data entry into the new registry. The certification is offered online through web-based study.
In summary, the MBS AQIP accreditation requirement for the database are as follows: 1) each program must assign a single data Bariatric Surgery Clinical Reviewer and 2) surgeons and NP/PAs involved directly in patient care cannot enter data into the BSCN database. In addition, programs will be encouraged to assign the role of data collector to medically trained personnel or to an experienced chart abstractor.
This will change the method of data abstraction. BSCOE participants have implemented a variety of data collection practices, including the following:
• Real-time entry of data into the BOLD software during patient visits
• Completion of encounter forms during patient visits with later transfer of the data to BOLD software
• Chart abstraction
• Third-party electronic health record (EHR) submission of data.
Going forward, the preferred practice of data collection for the ASMBS/ACS BQIP will be chart abstraction. Current training on the BSCN database focuses heavily on accurate chart abstraction and matching of clinical situations to definitions. For example comparing the clinical data for a surgical site infection (SSI) with a clear definition in order to determine if an SSI event has actually occurred. Ample practice cases are provided in the certification training. Because 30-day and long-term follow up are still required, collaboration between the surgeon practice and facility will be required to assure the accuracy and collection of these longer-term data points.
Inadequate training of data entry personnel. Although definitions of all BOLD data elements have always been provided as a downloadable PDF document within the software, in-depth, data-entry training focused on how to enter specific types of information in BOLD has never been widely available to BSCOE participants. A BOLD software manual has also never been provided to data-entry personnel. This has led to variations in the interpretation of data definitions. Questions regarding the assessment of comorbidity severity using the comorbidity scale and how to enter complications and revisional procedures in BOLD were very common to Surgical Review Corporation (SRC) support. Written guidelines on how to enter complications in BOLD have been provided but not until March 2011. Adverse events were often written out and not tied to specific definitions or CPT codes leading to increased variability. For example, in a recent evaluation of BOLD by the University of Michigan team led by John Birkmeyer, MD, bleeding after surgery was not able to be used for risk adjustment because of problems with the way the data was recorded. Differences in the interpretation of data definitions among BSCOE participants may potentially result in large variations in reported outcomes among BSCOE programs.
Non-standard data definitions. The comorbidity severity scale used in BOLD has been used primarily for research studies (Longitudinal Assessment of Bariatric Surgery) and conducted in restricted populations; BOLD is the first large data registry that has employed the scale. The scale is difficult to crosswalk with standard electronic medical record (EMR) definitions and with administrative databases. The list of complications in BOLD is broad, encompassing more than 140 events selected based on their known association with bariatric surgery; however, most have no impact on risk adjustment. None of the most recent definitions of these events indicates a level of severity of the event such as “severe” bleeding. In fact, postoperative hemorrhage is so variable that it could not be used for risk adjustment of the BOLD data set. BSCOE participants have been expected to report all complications that require “treatment,” including administration of prescription medications outside of standard postoperative care. This is unlike most if not all other data registries, which require reporting of only those complications, a hospital readmission, or a reoperation. This has likely led to differences in interpretation of when an event must be reported. The lack of standard data definitions in BOLD may increase data entry burden as special consideration must be given to BOLD data definitions which are not equivalent with other standard data collection efforts. The more involved the data collection is, the poorer the data especially as a patient moves away from the initial surgical experience.
While it is relatively straightforward to transfer demographic data into the data registry, the critical step in accuracy of the data is the assignment of a particular adverse event. Comparing the data in the medical record to the data definitions in the registry and making a decision to enter that particular adverse event to a particular patient is the heart of the clinical data base and the accuracy and strength of the database is related directly to this all-important function. Building an interface that allows demographic data to be entered will be possible very soon, but building a correlation between the data definitions and EHR/EMR-type systems will take some time and may not be achievable in an automated fashion.
Lack of sensitivity of the comorbidity severity scale. The use of the comorbidity severity scale rather than conventional objective measures to assess changes in the status of certain comorbidities may underestimate the percentage of patients whose disease has gone into remission at a given time after bariatric surgery. Specifically, the current severity scale indicates improvement in some comorbidities only when there is a major change in the type of treatment, such as whether medications are required. For example, patients with diabetes may decrease the number of oral medications they take from two to one, with a marked improvement in HbA1C, without improving their severity score. Likewise, it is not uncommon for patients whose hypertension or increased serum cholesterol has normalized as a result of weight loss after surgery to be maintained on low-dose, antihypertensive medication or statins for an indefinite time as a precautionary measure. As defined by the comorbidity severity scale, these patients would meet the criteria of a level 3 disease state when they have substantially improved their comorbidity burden.
Potential under-representation of complications. Surgical practices have been responsible for entering all post-discharge data, including complications, even if they were managed by another healthcare provider or at another facility. While laudable as a goal, it is impractical and impossible to actually execute. More importantly there is no practical audit process able to be performed to confirm the data or lack of data. Therefore, post-discharge complications may potentially be under-represented in the database. The BSCOE program did not designate or deny centers based on an outcomes-based requirement, although programs were denied when they failed to report complications that were uncovered during random chart review and seen on a greater scale during a 100-percent chart review during the three-year site visit.
In the new registry, follow-up data are required at visits occurring within 30 days, at 6 and 12 months, and annually. Complications after 30 days are limited to those resulting in a readmission or reoperation. Current procedural terminology (CPT) codes are used. This is a critical point as it allows for correlation with the publicly reported administrative data in the institution. Eventually, using these administrative databases may be one method of obtaining long-term follow up so making sure there is accurate coding is crucial.
Variations in the time to data entry. There has never been a required time frame for which data must be entered into BOLD following a patient visit. Differences in data entry workflow across programs have led to wide variations in the time to data entry by program and by visit type (i.e., preoperative vs. intraoperative vs. postoperative). At a given point in time, the follow-up data may appear to be incomplete for some patients owing to delayed data entry.
Moving forward, the MBS AQIP program database will require that data be entered within 120 days of the targeted follow-up period. At the close of the 120-day window, the database is locked for that particular follow-up record. All programs will enter data from March 1, 2012 and will be required to complete the data from March 1 within 120 days (June 29, 2012).
Frequency of on-site data auditing. The current practice of on-site data auditing, which occurs approximately every three years as part of site inspection, may not be sufficient to detect program-specific issues and to keep programs honest. Many other registries randomly audit a specific percentage of programs annually to improve overall accuracy of data collection. In addition, newer data registries have the capability of auditing against hospital records to determine accuracy.
Thoroughness of data auditing. BOLD data auditing has been limited to surgeries performed during a one-year period preceding the site inspection and has been focused on the following subset of data elements: procedures, complications, readmission, reoperations, and transfers. Under normal circumstances, approximately 10 percent of cases have been selected for random chart review. If unreported events are found, a 100-percent chart review may be triggered. Inconsistencies noted during site inspection are reported to Bariatric Surgery Review Committee (BSRC). This level of data audit may miss the two years of unaudited data from any program in the three-year cycle.
A quality loophole. One of the most important problems with the data collection occured because the program certified both facilities and surgeons, and some surgeons in a facility elected not to participate. This meant that there was a portion of the cases at the facility that were not audited except the year of the site visit since only the ASMBS BSCOE surgeons were required to put their data into BOLD. The facility only had to present the data from all surgeons for the purpose of the site visit but these additional cases were not audited. This weakens the reliability of the designation in a fundamental way and is why ASMBS chose in the unification with ACS to accredit the facility. All surgeons have to be part of the reporting going forward.
Inconsistent follow-up intervals among programs. Requirement 10 for the BSCOE program indicates that all programs must demonstrate a plan for obtaining follow-up data on 75 percent of their patients at 5 years post-surgery. For the BSCOE program, follow-up visits have been recommended, but not mandated at one, three, six, and 12 months within the first year following surgery and annually thereafter. Although most bariatric programs assess patients within 30-days following surgery, follow-up frequency varies substantially among BSCOE programs. Therefore, in order to report follow-up data beyond 30 days, visit windows must be wide to include all follow-up data available. For example, in a recent analysis the one–year follow-up window encompassed 6 to 18 months, with the follow-up visit closest to 12 months.
Incomplete follow-up data. BOLD has not had a follow-up tracking report that informs programs of which patients are due for follow-up visits when. BOLD has also not permitted the tracking of attempts by the bariatric program to contact patients and determining whether patients are truly lost to follow up. Thus, for the purposes of BOLD, only patients that die are considered lost to follow up and all other patients are considered eligible for follow up. In BOLD, approximately 66 percent of the patients were consented for research, so the follow up at one year was some subset of 66 percent. In published MBS data, the lack of transparency around the number of patients followed at reported time frames is valid. If only 23–40 percent of consented patients are reported on at one year, the validity of any one year data is called into serious question.
Inadequate feedback to programs through BOLD reports. The BOLD reports provided to date have not shown a program’s risk-adjusted outcomes versus national risk-adjusted benchmarks nor have they presented program data in a useful format (e.g., comorbidity data). This has limited the usefulness of BOLD data for quality improvement or even for use in the annual request for applications (RFAs) for insurance companies.
The database that will be used for the MBS AQIP program is a second-generation effort by the ACS and has the advantage of being informed by the NSQIP program, considered the strongest data available in surgery. Second generation registries mean the original data set was evaluated to see what data were needed to follow quality and data that were not needed were eliminated. This gives the programs a more sparse and pared down number of elements to report enhancing the likelihood of collecting better data. For instance, reporting of comorbitities were reduced from 33 to 18 and simple yes/no answers (including questions on medication). This also lessens the amount of time required for entry.
What will happen to the BOLD data? Clearly after acknowledging the limitations that have been described here, the BOLD data set still represents a large database of patients that have been entered. Demographic data are valid in this data set, but data around numbers of adverse events or long-term outcomes are more questionable for the reasons outlined above. A few papers have been published using BOLD data. The ASMBS will receive a “limited” BOLD data set (which means specific patient identifiers—the patient name or chart number—have been eliminated) on April 15, 2012. It will contain all the data that has been entered by programs/surgeons through March 31, 2012. ASMBS intends to do the following with that data:
1. Return the data to each surgeon/program in a dataset that can be used to answer RFAs from insurance companies and for a baseline dataset for the program. The goal is to return this data by the first National MBS Quality Forum on Friday, June 22, 2012 in San Diego, California at the annual ASMBS meeting. The society is working through a process now to define what data will be needed, who should analyze it, and how to best get that data to the programs/surgeons.
2. Make available a public-use file for researchers and program participants. This will be monitored through the research committee.
3. Prepare a state-by state-comparison with the aggregate BOLD data so that it can be used in access to care battles and posted on the ASMBS website.
4. Ensure that papers in progress that were begun using the BOLD data set can be completed.
Although it is impossible to answer or address all the issues or concerns that will come up over the next 90 days as we all transition (my program included) into the new database, this analysis provides some background about the transition and the basis for the decision to use one unified database for the new MBS AQIP program. As each program comes up into the new database there will be many questions and queries. A team of people will be available to make sure each question is addressed.
It is a remarkable achievement that community and academic surgeons alike embraced the collection of their data. Each of us must make a commitment to ensure the highest quality of data can be collected and the program must ensure that the data is available in an appropriate way to provide feedback to the programs and surgeons who enter it to improve patient safety and enhance the value (outcomes/cost) of MBS.
Acknowledgment: This article was developed in part from an analysis of BOLD performed by Debbie Winegar, PhD. Dr. Winegar served as the Senior Director of Research at Surgical Review Corporation from 2009 to 2012.
References
1. Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012 Mar 26. [Epub ahead of print]
2. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012 Mar 26. [Epub ahead of print]
3. Friedman MN, Sancetta J, Macgovern GJ. The amelioration of diabetes mellitus following subtotal gastrectomy. Surg Gynecol Obstet. 1955;100(2):201–204.
4. Pories WJ, Caro JF, Flickinger EG, Meelheim HD, Swanson MS. The control of diabetes mellitus (NIDDM) in the morbidly obese with the Greenville gastric bypass. 1987. Ann Surg. 206(3): 316–323.
5. Dixon JB, Zimmet P, Alberti KG, Rubino F. Bariatric surgery: an IDF statement for obese Type 2 diabetes. Diabet Med. 2011; 28:628–642.
6. Dixon JB, O’Brien PE, Playfair J, et al. Adjustable gastric banding and conventional therapy for type 2 diabetes: a randomized controlled trial. JAMA. 2008;299:316–323.
Category: ASMBS News and Update, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}