
Is There Room for Functional Foods and Phyto Supplements in the Bariatric Patient Population?
by Silvia Leite Faria, MSc, RD, PhD; Orlando Pereira Faria, MD; Fernanda Prates, and Larissa Berber
Silvia Leite Faria, MSc, RD, PhD, Orlando Pereira Faria, MD, Fernanda Prates, and Larissa Berber are from Gastrocirurgia de Brasília, Brazil. Dr. S. Faria is also a researcher at the University of Brasilia, Nutrition Department, Brazil.
Bariatric Times. 2015;12(9):13–16.
ABSTRACT
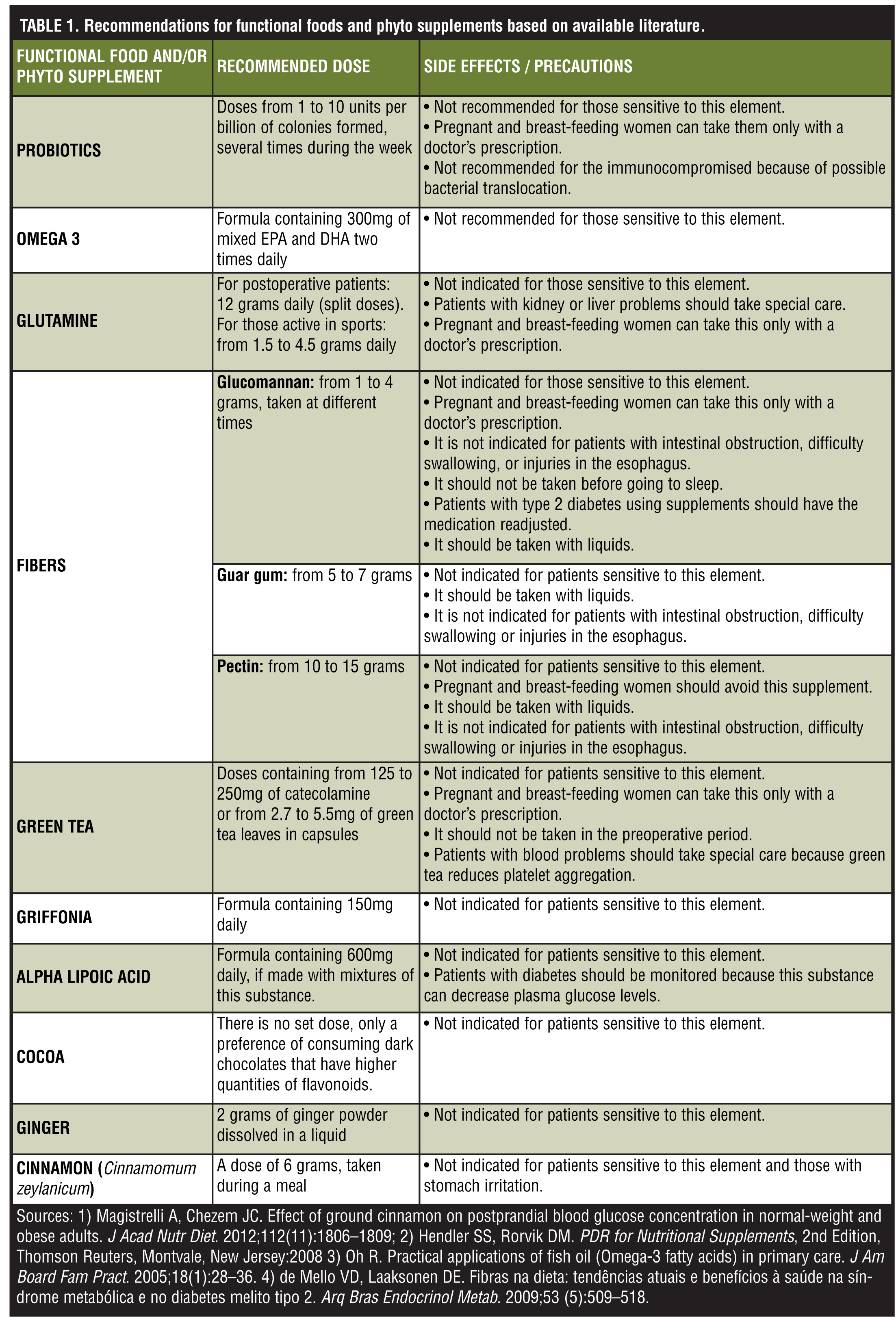
Functional foods and phyto supplements have been shown to improve weight loss and help with weight maintenance, making them an option for patients with overweight and obesity. In this article, the authors review functional foods and phyto supplements, including probiotics, omega 3, glutamine, fiber, green tea, griffonia, alpha lipoic acid. They also discuss thermogenic foods, including cocoa, ginger, and cinnamon. Functional foods and phyto supplements provide an auxiliary tool that healthcare professionals may use to help promote satiety, energy balance, fat oxidation, and improved nutrition in their bariatric patients. The authors conclude that while functional foods and phyto supplements cannot take the place of vitamin and mineral supplementation, they may help to improve body weight and nutritional status in certain patients.
Introduction
Bariatric surgery is currently one of the best tools for the treatment of obesity. Among the various surgical procedures performed, the most common are Roux-en-Y gastric bypass (RYGB), sleeve gastrectomy, and adjustable gastric band, all of which are malabsorptive and produce metabolic changes.[1]
Patients experience physiological and absorptive changes after undergoing these types of operations, and it is important that members of the multidisciplinary team have a plan for proper nutritional management. Postoperative care should aim to improve the clinical state of the patient and aid in weight loss and postoperative processes. While vitamin, mineral, and protein supplementation is well established and essential to this weight loss surgery patient population,[2] supplements based on functional food and phyto supplements have also shown some beneficial and effective results.[3–5]
By definition, functional foods are those that present physiological and metabolic health benefits not only in the prevention, but also in the treatment of diseases.[6,7]
Recent studies[8] have shown a correlation between functional foods and the prevention or treatment of chronic diseases, such as obesity. Functional foods have been found to be helpful in influencing the balance between energy expenditure and dietary intake. They are also helpful in other ways, such as decreasing total cholesterol levels, increasing high-density lipoprotein (HDL) fraction, and providing aid in intestinal transit.[9]
In this article, we review the utility and safety of functional foods and phyto supplements and discuss some of the most popular and available ones used among the bariatric population. See Table 1 for our recommendations and side effects/precautions in using these foods and supplements.
Methods
We conducted a literature search via the Medline, PubMed, Lilacs, and Cochrane databases using the following search terms: “bariatric surgery,” functional foods,” “phyto supplements,” “obesity and functional food,” and “Roux-en-Y gastric bypass.” Articles published before the year 2000 were excluded.
From the remaining articles, we determined which functional foods and phyto supplements we found to be most relevant among patients with obesity and/or those patients who had undergone bariatric surgery. These foods and supplements are as follows: 1) probiotics, 2) omega 3, 3) glutamine, 4) fiber, 5) green tea, 6) griffonia, 7) alpha lipoic acid, and 8) thermogenic foods and supplements (green tea, cocoa, ginger, and cinnamon).
Functional Foods and Supplements
Probiotics. According to the World Health Organization (WHO), probiotics are living organisms that, in determined quantities, can benefit human health.[10] Studies have shown that probiotics are useful in the treatment of metabolic and inflammatory disorders.[11]
Intestinal dysbiosis is a risk factor that may cause metabolic disorders, such as obesity, and is directly linked to an individual’s diet. Intestinal flora is made up of gram-negative and gram-positive bacteria living in symbiosis within the host, which is, in this case, a human being. When short-chain fatty acids are produced from hydrolysis and fermentation of polysaccharides (fibers), they tend to cause a balance of gut microbiota, which increases their sensitivity to the immunological system, decreases inflammation, and contributes to decreased appetite. This is due the release of glucagon-like peptide-1 (GLP-1) and peptide YY. Furthermore, the short-chain fatty acids influence lipid metabolism, which increases lipogenesis and decreases lipid oxidation.[12]
Le Chatelier et al[13] examined gut microbial genes and gut bacterial richness among a population sample of 123 individuals without obesity and 169 individuals with obesity. They found that individuals with a low bacterial richness were characterized by more marked overall adiposity, insulin resistance, and dyslipidaemia and a more pronounced inflammatory phenotype when compared to individuals with with high bacterial richness.
These facts have been elucidated in a study with mice.[14] In this study, mice with normal gut microbiota received a transplant of microbiota from obese mice. The researchers noted that the weight of the mice with transplants increased by 57 percent, and within two weeks the transplant mice developed insulin resistance.
The RYGB promotes changes in the composition of the patient’s microbiota.[15,16] RYGB seems to influence the increase of pathogens bacteria, such as Escherchia coli, and the decrease of beneficial bacteria, such as Lactobacilli and Bifidobacteria.[15] This change in gut microbiota may be due to the typical postoperative diet of the weight loss surgery patient, which is higher in protein and fat, and subsequently increased amounts of bacteria, than the preoperative diet. Another explanation would be that the postoperative intestinal anatomy of a weight loss surgery patient provides a favorable environment for the growth of bile-resistant proteobacteria, which may lead to an increase in primary bile production induced by incretin signaling via TGR5, a membrane-bound bile acid receptor well known for its roles in regulation of energy homeostasis and glucose metabolism.[17,18]
A study by Sweeney and Morton[17] examined patients who underwent bariatric surgery and were 3 to 6 months postoperative. Compared to the control group, the patients who underwent bariatric surgery showed a reduction of bacteria of the phylum Firmicutes in proportion to Proteobacteria.
Other studies have revealed that probiotic supplementation of different strains of bacteria resulted in loss of weight and fat, among other metabolic improvements.[14]
Omega 3. Omega 3 (polyunsaturated fatty acid) has anti-inflammatory properties and may assist in preventing or reducing weight gain following bariatric surgery. Omega 3 works by reducing the fat cell size. Large fat cells influence high fat oxidation, decreases the lipogenesis, and the synthesis of triglycerides.[7,19]
There are three types of omega 3 present in our diet: 1) eicosapentaenoic acid (EPA), 2) docosahexaenoic acid (DHA), and 3) alpha-linolenic acid (ALA). EPA and DHA are obtained through the intake of fatty fish and ALA is obtained through vegetable oils.
The typical nutritional composition of the diet of patients with overweight or obesity is high levels of fat, especially saturated fat and trans fat, which have been shown to downshift the satiety mechanism. Furthermore, high levels of saturated fatty acids activate the innate immunological system, which may cause inflammation of tissue and insulin resistance.[19,20] Studies[19,21] have shown that daily omega 3 supplementation in patients with obesity can increase weight loss and satiety while reducing caloric intake.
The effect of omega 3 on weight loss may be due to its stimulation of secretion of cholecystokinin in a more efficient manner than omega 6.[20] One such means of omega 3 supplementation is via ALAs, found in linseed oil, soy beans, and nuts. ALA is easily converted into two active products, docosahexaenoic acid (DHA) and eicosapentaenoic acid (EPA). We believe that supplementation in capsule form is best because through this vehicle, omega 3 is available in the form of micelles, which facilitates the absorption of lipids. This is an important consideration in RYGB patients because the surgery may hinder the absorption of fats including omega 3.[22]
Glutamine. The body contains high levels of concentrated glutamine, a nonessential amino acid that acts as an immune regulator. It is involved in various metabolic functions, making it a biochemical precursor of proteins, amino acids, and nucleic acids. Studies have shown that glutamine is one of the preferred fuel sources for the small intestine and is essential for epithelial growth.[23] Glutamine stimulates the growth of intestinal cells in isolated areas and also increases the surface and the jejunal absorption area.[23]
Bariatric operations, such as RYGB and LSG, that change the anatomy of the digestive system, may cause patients to have poor absorption of micronutrients and macronutrients in the postoperative period. Patients may also experience nutritional deficiency and weakness of the immune system after these operations. According to Quan et al,[5] major trauma or surgery to the intestinal region can cause damage to the intestinal mucosa and decrease of permeability, which could promote the entry of bacteria and other micro-organisms into the bloodstream.[5] This bacterial translocation can lead to infection or more serious diseases. This study also examined the effects of glutamine on the change of intestinal permeability and its relationship to systemic inflammatory response in early abdominal postoperative patients. The authors concluded that glutamine may maintain intestinal barrier and attenuate systemic inflammatory response in early postoperative patients.
In studies of postoperative RYGB patients, the daily use of glutamine has been shown to promote a reduction of the expression of pro-inflammatory markers, such as C-reactive protein and interleukin-6.[24] Moreover, glutamine has an anti-catabolic (i.e., prevents or minimizes the breakdown of hard-earned muscle) characteristic that neutralizes the catabolism effect caused by cortisol in situations of stress and exercise. This may help with weight loss by improving fat mass and maintenance of muscle mass.[25–27]
Phyto Supplements
Fiber. Fiber is the edible part of plants that behaves as nondigestible carbohydrates. Fiber is not absorbed by the small intestine, but rather undergoes fermentation in the large intestine. Fiber can perform as a laxative by reducing levels of serum glucose and cholesterol. There are two types of fiber: soluble and insoluble.[25] Soluble fiber helps to reduce low density lipoproteins (LDL) cholesterol and triglycerides. Insoluble fiber helps in forming of the stool and facilitating intestinal transit. Both types of fiber contribute to the formation of a healthy intestinal flora and can reduce the absorption of calories.[7]
Studies demonstrate an inverse relationship between fiber intake and body weight, revealing that diets rich in fiber (in the form of food or supplementation) may help individuals reduce their body weight. Fiber forms a bulking gel in the intestine, which changes the viscosity of gastric contents. This aids the intestinal transit and response to insulin, modulating satiety of the individual.[9,28]
Glucomannan, classified as a soluble fiber, is found in a species of the Konjac plant in China and Japan. Studies using glucomannan supplementation have shown mixed results for weight loss; however, one randomized, controlled trial[29] demonstrated greater weight and fat mass loss in individuals who took soluble fiber supplements compared to those that had a low-fiber diet.
Studies within the bariatric population have shown good results with glucomannan in preventing dumping syndrome,[30] which is common in the weight loss surgery population.[31]
It is important to note that glucomannan may cause a bezoar effect in some patients, especially in patients with difficulty swallowing or injuries of the esophagus, and low ingest of liquids.[32] To prevent this problem, we advise patients to take glucomannan and all other fiber supplements with an adequate quantity of liquids.
Pectin, another type of soluble fiber, is found in most plants, but has higher concentrations in apples and citrus fruits. Pectin is also available in supplement form (powder and capsule).
For the bariatric patient population, fiber supplementation may be used for different reasons, including the following: 1) to achieve the adequate amount of fiber needed in the postoperative diet; 2) to increase satiety, and 3) to help prevent late dumping syndrome, which is common in bariatric patients.
Fiber supplements may be used with meals in order to decrease the pace in which food travels through the gastrointestinal tract.[33] We recommend the following to our patients in split doses: guar gum (500mg), glucomannan (500mg), and pectin (500mg).
Among patients who have experienced weight regain after bariatric surgery, the literature shows that 15 grams of soluble fiber can be used with a low glycemic load diet with good results for excess weight loss.[34] Additional studies show that bariatric patients who are 1 to 2 years postoperative have a fiber intake less than what is recommended.[35,36]
Green tea. Green tea’s benefits come from its chemical composition of various types of polyphenols. Polyphenols are types of anti-oxidants, with proven beneficial effects in preventing and treating certain types of inflammation, cancer, cardiovascular diseases, and obesity.[37]
Green tea can be consumed in liquid form, leaves, and/or capsules. For the bariatric population, we prefer capsule supplementation because it ensures the patient receives the adequate quantity. We recommend 125 to 250mg of catecolamine or 2.7 to 5.5mg of green tea leaves in capsule form.
The polyphenol attributed to weight loss is epigallocatechin gallate (EGCG). It acts on suppression of adipocyte differentiation and proliferation, inhibition of fat absorption by the intestinal microflora, and suppression of catechol-o-methyltransferase enzyme (COMT), which is responsible for fat oxidation in the brown adipose tissue.[9,38,39]
Dulloo et al[40] concluded that green tea has thermogenic properties and promotes fat oxidation beyond that explained by its caffeine content per se. The green tea extract may play a role in the control of body composition via sympathetic activation of thermogenesis, fat oxidation, or both.[40]
It is important to note that green tea should be consumed with caution because high doses can cause liver toxicity, inflammation, and liver damage.[41–43]
Griffonia. Griffonia is a substance that comes from a plant of African origin called Griffonia simplicifolia. It is the precursor of a substance called 5-hydroxytryptophan (5-HTP), in which the human body contributes to the formation of serotonin.[44] In addition to being an effective treatment for depression, it has been shown to have beneficial effects on weight loss.[33]
In the weight control process, griffonia’s mechanism of action is correlated with the function of serotonin, which in addition to regulating appetite and reducing food intake, may be linked to increased levels of leptin. In studies with mice, 5-HTP administrations resulted in increased leptin. In a study of overweight women in which griffonia was administered for one month, the supplement showed a significant change in body composition.[45]
There are no studies among bariatric patients demonstrating the use of griffonia, but the success obtained in nonobese models suggests that implementing its use as part of postoperative treatment in weight loss surgery patients may be beneficial.
Alpha lipoic acid. Alpha lipoic acid (ALA) is found in both plant and animal sources. Most of its mechanisms of action are related to oxidative reactions that occur in the mitochondria. In weight management, ALA helps with the activated protein kinase channel (AMPK), the inhibition of the factor nuclear kappa B (NF-κB), and the differentiation of adipocytes.[33]
The results of several studies corroborate the use of ALA as a potential treatment for obesity. Effects of ALA supplementation are as follows: weight reduction, decrease of LDL, reduction of serum levels of free fatty acids, and reduction of pro inflammatory cytokines, such as interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α).[46,47]
Thermogenic Foods
Foods that are classified as thermogenic are foods that require more energy and work than typically expended to be digested and absorbed. This means the body expends more energy digesting the food than the food provides the body as energy, thus burning calories in the process, which is composed of a series of reactions (i.e., ingestion, digestion, and absorption). Compared to regular food digestion, which represents 5 to 10 percent of the total energy expenditure, thermogenic food represents a greater percentage of total energy expenditure.[48,49] Table 1 lists the following thermogenic foods: green tea, cocoa, ginger, and cinnamon, and our recommendations for their use.
Green tea. Green tea extract, which contains both caffeine and catechin polyphenols, is considered a thermogenic food. Caffeine is a sympathetic nervous system stimulant known to increase energy expenditure. Green tea in particular has been shown to increase daily energy expenditure by four percent.[40]
Cocoa. Cocoa is rich in flavonoids and is widely used in medical treatment of cardiac diseases and in the prevention of cancer.[50] Furthermore, the use of cocoa reduces the production of inflammatory molecules species reactive to oxygen, reduces the expression of various genes associated with the transport of fatty acids and their synthesis in the liver and mesenteric, and increases expression of genes associated with thermogenesis.[51,52] Procyanidin, which is present in cocoa, has the ability to modulate TNF-α and this induces NF-κB, a cytokine transcription factor.[53]
Ginger. Ginger, which is also rich in flavonoids, is proposed to have anti-inflammatory and antihypertensive properties, as well as effects on insulin sensitivity and stimulating peristalsis and the secretion of gastric juice.[54]
In some studies with mice, there is evidence that ginger aids in weight loss, decreasing levels of glucose, insulin, and total cholesterol, in addition to increasing high density lipoproteins (HDL) serum levels.[54,55]
Cinnamon. Studies in vitro and in vivo demonstrate that cinnamon has a sensitizing effect on insulin and may be used to control diseases, such as type 2 diabetes.[55,57] Cinnamomum zeylanicum or ceylon cinnamon, which is considered to be “true” cinnamon, has been found to help in reducing hunger, lowering the atherogenic effects of LDL, and reducing insulin levels, providing homeostasis of glucose.[58] It is important to note that all types of cinnamon contain coumarins, which in high doses have potentially toxic effects on the liver.59 The coumarin content in Ceylon cinnamon appears to be lower than in other types, such as Cinnamomum aromaticum or Chinese Cassia. It is important to recommend the correct form of cinnamon to patients.
Conclusion
The routine vitamin and mineral supplementation has already been established for the bariatric patient population.[2] The use of functional foods and phyto supplements should not replace this established supplementation; however, they may be used in some patients to improve nutritional deficiencies and weight loss and/or weight maintenance. The functional foods and phyto supplements discussed in this article are listed in Table 1.
Some functional foods and/or phyto supplements can be used among the bariatric population without modifying the established routine of mineral, vitamin, and protein supplementation. The nutritionist/dietitian should take care to prescribe supplements in adequate doses and avoid high dosages that have not been tested among bariatric and/or patients with obesity. Cost of these supplements is another area of consideration. Healthcare providers should emphasize that routine supplementation takes precedence over functional foods/phyto supplements when budget is a concern.
Some supplements may help control important parameters, such as the lipid profile and the composition of intestinal flora of patients. While our literature search produced useful articles, we found a lack of evidence on the use of functional foods and phyto supplements among the bariatric population. We believe that more studies are needed to clarify effects and recommendations for these functional food and phyto supplements in patients with obesity, especially those who have undergone malabsorptive bariatric surgery.
References
1. Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg. 2013;23(4):427–436.
2. Aills L, Blankenship J, Buffington C, Furtado M, Parrott J. ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient. Surg Obes Relat Dis. 2008;4(5 Suppl):S73–108.
3. Woodard GA, Encarnacion B, Downey JR, et al. Probiotics improve outcomes after Roux-en-Y gastric bypass surgery: a prospective randomized trial. J Gastrointest Surg. 2009;13(7):1198-204.
4. Gargallo Fernández MM, Breton LI, Basulto MJ, et al. Evidence-based nutritional recommendations for the prevention and treatment of overweight and obesity in adults (FESNAD-SEEDO consensus document). The role of diet in obesity treatment (III/III). Nutr Hosp. 2012;27(3):833–864. [Article in English, Spanish],
5. Quan ZF, Yang C, Li N, Li JS. Effect of glutamine on change in early postoperative intestinal permeability and its relation to systemic inflammatory response. World J Gastroenterol. 2004;10(13):1992–1994.
6. Ferrari CKB, Torres E. Alimentos funcionais: quando a boa nutrição melhora a nossa saúde. Educação alimentar. Revista Portuguesa de saúde pública. 2002;20(2): 31–34.
7. Varo D. Alimentos Funcionais: Faça do Alimento Seu Medicamento e do Medicamento, Seu Alimento. Editora Artes e ofícios. Porto Alegre, Rio Grande do Sul, 2006:58–60; 62–70.
8. Basho SM, Bin MC. Properties of functional foods and their role in the prevention and control of hypertension and diabetes. Interbio. 2010; 4(1): 48–58.
9. Costa Neusa M. Rosa C. Alimentos Funcionais., Editora Folha de Viçosa, Minas Gerais, 2006: 115–130.
10. Joint Food and Agriculture Organization of the United Nations/World Health Organization Working Group report on drafting guidelines for the evaluation of probiotics in food, London, Ontario, Canada, April 30 and May, 2002.
11. Hur KY, Lee M-S. Gut Microbiota and Metabolic Disorders. Diabetes Metab J. 2015;39(3):198–203.
12. Festi D, Schiumerini R, Eusebi LH, et al. Gut microbiota and metabolic syndrome. World J Gastroenterol. 2014;20(43):16079–16094.
13. Le Chatelier E, Nielsen T, Qin J, et al. Richness of human gut microbiome correlates with metabolic markers. Nature. 2013;500:541–546.
14. Prados-Bo A, Gómez-Martínez S, Nova E, Ascensión M. El papel de los probióticos en el manejo de la obesidad. Nutr Hosp. 2015;31(Supl. 1):10–18.
15. Furet JP, Kong LC, Tap J, et al. Differential adaptation of human gut microbiota to bariatric surgery-induced weight loss: links with metabolic and low-grade inflammation markers. Diabetes. 2010;59(12):3049–3057.
16. Tremaroli V, Karlsson F, Werling M, et al. Roux-en-Y gastric bypass and vertical banded gastroplasty induce long-term changes on the human gut microbiome contributing to fat mass regulation. Cell Metab. 2015; 22(2): 228–238.
17. Sweeney TE, Morton JM. Metabolic surgery: Action via hormonal milieu changes, changes in bile acids or gut microbiota? A summary of the literature. Best Pract Res Clin Gastroenterol. 2014;28(4):727–740.
18. Thomas C, Gioiello A, Noriega L, et al. TGR5-mediated bile acid sensing controls glucose homeostasis. Cell Metab. 2009;10(3):167–177.
19. Belchior T, Paschoal VA, Magdalon J, et al. Omega-3 fatty acids protect from diet-induced obesity, glucose intolerance, and adipose tissue inflammation through adipose tissue inflammation through PPARγ-dependent and PPARγ-independent actions. Mol Nutr Food Res. 2015;59(5):957–967.
20. Benites J, Cardoso J, Conti T, Martins J, Sonh V. Uso de alimentos termogênicos no tratamento da obesidade. 2010. Instituto de Nutrição Josué de Castro, Universidade Federal do Rio de Janeiro, Rio de Janeiro, 2010.
21. Golub N, Geba D, Mousa SA, Williams G, Block RC. Greasing the wheels of managing overweight and obesity with omega-3 fatty acids. Med Hypotheses. 2011;77:1114–1120.
22. Arnoldussen IAC, Kiliaan AJ. Impact of DHA on metabolic diseases from womb to tomb. Mar Drugs. 2014;12(12): 6190–6212.
23. Noth R, Häsler R, Stüber E, et al. Oral glutamine supplementation improves intestinal permeability dysfunction in a murine acute graft-vs.-host disease model. Am J Physiol Gastrointest Liver Physiol. 2013;304(7):G646–54.
24. Breitman I, Saraf N, Kakade M, et al. The effects of an amino acid supplement on glucose homeostasis, inflammatory markers, and incretins after laparoscopic gastric bypass. J Am Coll Surg. 2011;212(4):617–625; discussion 625–627.
25. Ray RM, Johnson LR. Regulation of intestinal mucosal growth by amino acids. Amino Acids. 2014;46(3):565–573.
26. Cukier C, Waitzberg DL, Borges VC, et al. Clinical use of growth hormone and glutamine in short bowel syndrome. Rev Hosp Clin Fac Med Sao Paulo. 1999;54(1):29–34.
27. Forti F, Cancelliero KM, Guirro R, da Silva. Efeitos da glutamina e da estimulação elétrica sobre o perfil metabólico dos músculos desnervados. Rev. bras. Educ. Phys. Esp, São Paulo. 2004;18(3):273–281.
28. Papathanasopoulos A, Camilleri M. Dietary fiber supplements: effects in obesity and metabolic syndrome and relationship to gastrointestinal functions. Gastroenterology. 2010;138(1):65-72.e1-2.,
29. Sood N, Baker WL, Coleman CI. Effect of glucomannan on plasma lipid and glucose concentrations, body weight, and blood pressure: systematic review and meta-analysis. Am J Clin Nutr. 2008;88: 1167–1175.
30. Tack J, Arts J, Caenepeel P, De Wulf D, Bisschops R. Pathophysiology, diagnosis and management of postoperative dumping syndrome. Nat Rev Gastroenterol Hepatol. 2009; 6(10):583–590.
31. Ukleja A. Dumping syndrome: pathophysiology and treatment. Nutr Clin Pract. 2005;20(5):517–525.
32. Vanderbeek PB, et al. Esophageal obstruction from a hygroscopic pharmacobezoar containing glucomannan. Clin Toxicol (Phila). 2007;45:80–82.
33. Hendler SS, Rorvik DM. PDR for Nutritional Supplements, 2nd Edition, Thomson Reuters, Montvale, New Jersey: 2008.
34. Faria SL, de Oliveira Kelly E, Lins RD, Faria OP. Nutritional management of weight regain after bariatric surgery. Obes Surg. 2010;20(2):135–139.
35. Jeffreys RM, Hrovat K, Woo JG, et al. Dietary assessment of adolescents undergoing laparoscopic Roux-en-Y gastric bypass surgery: macro- and micronutrient, fiber, and supplement intake. Surg Obes Relat Dis. 2012;8(3):331–336.
36. Novais PF, Rasera I Jr, Leite CV, et al. Food intake in women two years or more after bariatric surgery meets adequate intake requirements. Nutr Res. 2012;32(5):335–341.
37. Senger AEV, Schwanke C, Gottlieb M. Green tea (Camellia sinensis) and its functionals properties on transmissible chronic diseases. Scientia Medica (Porto Alegre). 2010; 20(4):292–300.
38. Meydani M, Hasan ST. Dietary polyphenols and obesity. Nutrients. 2010; 2(7): 737–751.
39. Fonseca-Alaniz M, Takada J, Alonso-Vale M, Lima F. The adipose tissue as a regulatory center of the metabolism. Arq Bras Endocrinol Metab São Paulo. 2006; 50(2): 216–229.
40. Dulloo AG, Duret C, Rohrer D, et al. Efficacy of a green tea extract rich in catechin polyphenols and caffeine in increasing 24-h energy expenditure and fat oxidation in humans. Am J Clin Nutr. 1999;70(6):1040–1045.
41 Bonkovsky HL. Hepatotoxicity associated with supplements containing Chinese green tea (Camellia sinensis). Ann Intern Med. 2006;144(1):68–71.
42. Mazzanti G1, Menniti-Ippolito F, Moro PA, et al. Hepatotoxicity from green tea: a review of the literature and two unpublished cases. Eur J Clin Pharmacol. 2009;65(4):331–341.
43. Church RJ, Gatti DM, Urban TJ, et al. Sensitivity to hepatotoxicity due to epigallocatechin gallate is affected by genetic background in diversity outbred mice. Food Chem Toxicol. 2015;76:19–26.
44. Hara R, Kino K. Enhanced synthesis of 5-hydroxy-l-tryptophan through tetrahydropterin regeneration. AMB Express. 2013; 3: 70.
45. Rondanelli M, Opizzi A, Faliva M, Bucci M, Perna S. Relationship between the absorption of 5-hydroxytryptophan from an integrated diet, by means of Griffonia simplicifolia extract, and the effect on satiety in overweight females after oral spray administration. Eat Weight Disord. 2012;17(1):e22–28.)
46. Gomes MB, Negrato CA. Alpha-lipoic acid as a pleiotropic compound with potential therapeutic use in diabetes and other chronic diseases. Diabetol Metab Syndr. 2014;6(1):80.
47. Fernández-Galilea M, Pérez-Matute P, Prieto-Hontoria PL, et al. Effects of lipoic acid on lipolysis in 3T3-L1 adipocytes. J Lipid Res. 2012;53(11):2296–2306.
48. Souza CL, Oliveira MRM. Factors related to the energetic metabolism in obesity. Nutrire. 2010;35(2): 145–164.
49. Vogel RM, Joy JM, Falcone PH, et al. Consuming the multi-ingredient thermogenic supplement for 28 days is apparently safe in healthy adults. Food Nutr Res. 2015;59:27999.
50. Galleano M, Oteiza P, Fraga C. Cocoa, chocolate and cardiovascular disease. J Cardiovasc Pharmacol. 2009; 54(6): 483–490.
51. Latif R. Chocolate/cocoa and human health: a review. Neth J Med. 2013;71(2):63–68.
52. Andújar I, Recio MC, Giner RM, Ríos JL. Cocoa polyphenols and their potential benefits for human health. Oxid Med Cell Longev. 2012;2012:906252.
53. Pérez-Cano FJ, Massot-Cladera M, Franch A, Castellote C, Castell M. The effects of cocoa on the immune system. Front Pharmacol. 2013;4:71.
54. Mansour MS, Ni YM, Roberts AL, et al. Ginger consumption enhances the thermic effect of food and promotes feelings of satiety without affecting metabolic and hormonal parameters in overweight men: a pilot study. Metabolism. 2012;61(10):1347–1352.
55. Mahmoud RH, Elnour WA. Comparative evaluation of the efficacy of ginger and orlistat on obesity management, pancreatic lipase and liver peroxisomal catalase enzyme in male albino rats. Eur Rev Med Pharmacol Sci.. 2013;17(1):75–83.
56. Vafa M, Mohammadi F, Shidfar F, et al. Effects of cinnamon consumption on glycemic status, lipid profile and body composition in type 2 diabetic patients. Int J Prev Med. 2012;3(8):531–536.
57. Sartorius T, Peter A, Schulz N, et al. Cinnamon extract improves insulin sensitivity in the brain and lowers liver fat in mouse models of obesity. PLoS One. 2014;9(3):e92358.
58. Ranasinghe P, Perera S, Gunatilake M, et al. Effects of Cinnamomum zeylanicum (Ceylon cinnamon) on blood glucose and lipids in a diabetic and healthy rat model. Pharmacognosy Res. 2012;4(2):73–79.
59. Ghosh P, Markin RS, Sorrell MF. Coumarin-induced hepatic necrosis. Am J Gastroenterol. 1997;92:348–9
FUNDING: No funding was provided.
DISCLOSURES: The authors report no conflicts relevant to the content of this article.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}