How to Perform a Gastrostomy
This column recruits expert surgeons to share step-by-step technical pearls on bariatric procedures.
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS, and Daniel B. Jones, MD, MS, FACS
This Month’s Technique: How to Perform a Gastrostomy
This Month’s Featured Experts: Emanuele Lo Menzo, MD, PhD, FACS, FASMBS, Staff Surgeon, The Bariatric and Metabolic Institute, Department of General Surgery, Cleveland Clinic Florida, Weston, Florida; Associate Professor of Surgery, Florida International University, Miami, Florida. Abraham Betancourt, MD, MIS/Bariatric Clinical Research Fellow, Bariatric and Metabolic Institute and Section of Minimally Invasive Surgery Dept. of General and Vascular Surgery, Cleveland Clinic Florida, Weston, Florida.
FUNDING: There was no funding for the preparation of this manuscript.
DISCLOSURES: The author reports no conflicts of interest relevant to the content of this article.
Bariatric Times. 2013;10(7):12.
Introduction
Although placement of a remnant gastrostomy tube at the time of gastric bypass is a technically easy procedure, its insertion later on could be challenging, especially in the setting of an ante-gastric Roux limb. The remnant gastrostomy tube can be utilized for decompression, but also as an access for feeding and endoscopic procedures. The acute decompression of the gastric remnant is necessary in the setting of functional or mechanical obstruction of the remnant, bilio-pancreatic limb, or common channel. Trans-remnant feedings are necessary in cases of gastrojejunal anastomosis problems (leaks or stenosis) or inadequate oral intake. Finally endoscopic access to the gastric remnant might be necessary to evaluate and treat upper gastrointestinal and biliary pathologies (bleeding, masses, choledocholithiasis, sphincter of Oddi dysfunction).
Several techniques have been described, and the choice depends also on the commercial gastrostomy kit available. Our preference is to use a standard 24 French foley catheter.
Surgical Technique:
Step 1: Selection of adequate location. The appropriate location of the gastrostomy is in the anterior wall of the body of the stomach. The tube should be 4 to 5cm proximal to the antrum to avoid gastric outlet obstruction by the inflated balloon. The stomach should be adequately mobilized in order to reach the anterior abdominal wall at least 2cm below the ribcage. If the procedure is done laparoscopically, additional distance from the costal margin should be obtained to account for the pneumoperitoneum. Division of the short gastric vessels is usually sufficient to provide adequate mobilization.
Step 2: Placement of the purse-string suture. Seromuscular bites of a 2-multifilament absorbable suture are utilized to prepare the purse string wide enough to accommodate the gastrostomy tube (Figure 1). The tails of the purse-string and are left long.
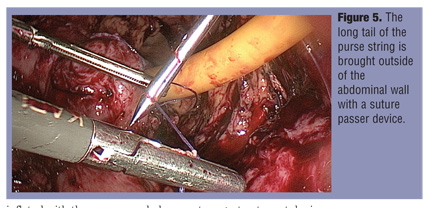
Step 3: Gastrostomy and tube placement. Using the energy device, the gastrotomy is made in the middle of the purse-stringed area (Figure 2). A 24 Fr gastric tube is inserted from the skin incision in the left upper quadrant, inserted in the stomach, and fed toward the pylorus (Figure 3). The balloon is inflated with the recommended amount (usually 20cc), the purse string tied, and gentle traction applied (Figure 4). The tube is tested with saline. The long tail of the purse string is brought out the abdominal wall using a suture passer device, and the stomach is gently pulled against the abdominal wall by tieng the suture above the fascia (Figure 5). The gastrostomy tube is kept to gravity drainage for 24 hours prior to being utilized.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}