Usefulness of Upper Gastrointestinal Contrast Studies in Post-Laparoscopic Roux-en-Y Gastric Bypass Surgery
by Holly M. Thompson, MD, MPH, and Robert A. Andrews, MD
Dr. Thompson, is from the Department of Surgery, Beth Israel Deaconess Medical Center, Boston, Massachusetts. Dr. Andrews is from the Department of Minimally Invasive Surgery, Beth Israel Deaconess Medical Center, Boston, Massachusetts.
Funding: There was no funding for the development of this article.
Financial Disclosures: The authors reports no conflicts of interest relevant to the content of this article.
Bariatric Times. 2010;7(8):10–14
Abstract
The laparoscopic Roux-en-Y gastric bypass is an effective intervention in treating class III obesity; however, new technologies come with the innate concern for detecting complications of which controversy exists regarding the usefulness of upper gastrointestinal studies. Due to the increasing number of bariatric patients and the associated cost of diagnostic studies, the authors felt it worthwhile to conduct a literature review to critically evaluate the debate surrounding the use of upper gastrointestinal studies. Their analysis supports the notion that clinical suspicion of the surgeon ought to be integrated into the decision management process prior to performing diagnostic tests. A prospective, randomized, controlled trial of routine versus selective upper gastrointestinal studies to detect leaks that evaluate the length of patient stay, hospital charges, patient discomfort, and confidence of changes in clinical decisions is needed to objectively evaluate data of the safety and efficacy of upper gastrointestinal studies studies in post-laparoscopic Roux-en-Y bypass surgery.
Introduction
When used correctly, diagnostic technologies either help support or negate a clinical suspicion or concern. There is a positive predictive value (PPV) and negative predictive value (NPV) associated with all diagnostic tests, which rely principally on the prevalence of the sought out disease or clinical suspicion in the tested population. Diagnostic tools are not intended to be used in isolation for confirmation or as a means to rule out a diagnosis; rather their value is in providing the practitioner with an increased level of confidence to facilitate patient management with the hope of obviating excess morbidity. The rapid advancement and adaptation of technology has provided medicine with outstanding imaging modalities with increased confidence of diagnosis and improvements in ease of use. As such, clinicians have become less confident with older technologies and clinical exam techniques and more reliant on advanced diagnostics. Increase in usage has increased the cost of diagnostic tests in healthcare, which may be justified in bariatric surgery. Upper gastrointestinal (UGI) studies have traditionally been used after laparoscopic Roux-en-Y gastric bypass (RYGB) in evaluation and documentation of postoperative anatomy and concern for complications, such as leaks. Nevertheless, much debate exists regarding the value of the perceived low technology test and in the growing environment of government healthcare, evidence-based medicine, and pressure to reduce cost, UGI studies have fallen under scrutiny.
Background
The landmark National Institute of Health 1991 consensus statement officially declared obesity a disease with severe long-term public health consequences. It also acknowledged surgery as a means to treat obesity and its power and role in limiting, and in many cases, preventing and reversing disease morbidity.[1–5] The laparoscopic RYGB operation has been shown to be safe and effective in treating obesity.[5,6] Recent studies have shown that the risk of death over time was reduced by 35 percent in individuals with severe obesity who underwent bariatric surgery when compared to those who did not.[7,8] The laparoscopic approach results in smaller incisions, less pain, faster recovery time, and shorter hospital stays without sacrificing weight loss benefits.[9,10]
Concern for Leaks
Surgery is not without its complications that can lead to increased morbidity, mortality, and costs.[11,12] Traditionally UGI studies have been routinely employed on postoperative Day 1 to evaluate the most dreaded and serious complication after gastric bypass surgery—the anastomotic gastrointestinal leak.[13–16] Leak is reported to occur in up to five percent of patients and is associated with a high rate of morbidity and mortality. Although overall risk of mortality after bypass surgery is less than one percent, at autopsy, leaks were perceived to be responsible for about 50 percent of deaths.[17] Almahmeed et al[18] demonstrated in a prospective study that anastomotic leaks significantly increased the risk of developing additional life-threatening complications, such as sepsis, renal failure, bowel obstruction, and internal hernia. Patients who develop leaks have significantly longer hospital stays than those without leaks, averaging 24.8 days compared to 3.0 days, respectively.[18] Fullum et al[39] reports that the mortality rate can be as high as 50 percent and the cumulative expense for a complicated leak can exceed $200,000. The grave concern and desire for early diagnosis has traditionally led to the use of UGI contrast studies to evaluate the surgical gastrojejunal anastamosis for occult leaks as well as surgeon-dependant placement of a surgical drain, or use of methylene blue or air insufflation tests.[19–22] Laparoscopy also imparts a challenging learning curve that further encourages the use of UGI studies after RYGB. Nevertheless, apprehension exists that a negative UGI study on postoperative Day 1 may inadvertently give a false sense of security and lead to a decrease in observation time and subsequent increase in severity of leak. A question remains whether this concern is bona fide as studies have shown that the incidence of leak does not differ from open versus laparoscopic RYGB.[23,24] Consequently, routine use of UGI studies has become controversial as the validity and precision of the test is brought into question given inconsistent statistical reports.[19,20]
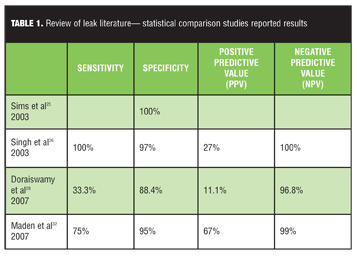
A screening tool with no false positive detection as reported by Sims et al[25] with 100-percent specificity implies that many cases are not identified. Studies with high sensitivity and low positive predictive value (PPV) emphasize the problem of high false positives—patients identified as having a leak who do not actually have one—with the routine use of postoperative UGI studies. This questions the management of such cases and the usefulness of substituting clinical markers as advantageous indicators in detecting leaks.
Clinical Indicators of Leaks
Postoperative leaks are traditionally thought to be difficult to recognize as clinical findings can be nonspecific and subtle in individuals with obesity. Tachycardia, fever, and abdominal pain are frequently encountered within the realm of the anticipated postoperative course in bariatric patients. Bariatric patients often experience respiratory insufficiency, atelectasis, and post-surgical abdominal pain.[20,29] Nevertheless, Kalakowski et al[30] reported in 2010 that clinical indicators of fever, tachycardia, and tachypnea, combined have a sensitivity of 58.33 percent and specificity of 99.75 percent of detecting leak. The study showed that although most patients had a heart rate exceeding 100 beats per minute, each patient who developed a leak had a heart rate of over 120 beats per minute, suggesting the worrisome nature of tachycardia during the postoperative course.
Causes of Leaks
In an effort to identify and target variables that cause leaks, Fullum et al[39] evaluated variables of intraoperative technique. In 2009, Fullum et al[39] conducted a study evaluating 760 patients. A linear staple line technique with hand sewing of gastrojejunostomy was performed as well as use of tension reduction sutures. Immediate intraoperative observance for detection of leak using methylene blue and air insufflation was performed. Of the 760 cases, four intraoperative leaks were detected and immediately fixed and no patient had leak on postoperative UGI study. Two patients who had a negative UGI study on postoperative Day 1 later developed leaks on postoperative Days 5 and 7. These patients were treated nonsurgically with percutaneous drainage, antibiotics, and total parenteral nutrition (TPN). This study and other studies[23,39–42] support the notion that early leaks, screened for with UGI studies, may actually be caused by technical error, which can be more appropriately identified immediately in the operating room.
Usefulness of UGI
Many institutions are reevaluating the routine use of UGI studies on postoperative Day 1. Doraiswamy et al[28] evaluated the management of patients with 1) normal UGI, 2) abnormal UGI not requiring intervention, and 3) abnormal UGI studies requiring intervention. Of the 560 patients evaluated, only 4.8 percent were found to have leaks by using a UGI study and required repeat imaging or re-operation. In their study, two of the three patients with gastrojejunal leaks had an initial negative UGI study supporting the limited usefulness of routine use on postoperative Day 1. White et al[31] compared routine versus selective use of UGI studies given clinical symptoms and found no statistical difference between the two groups or change in patient management from added UGI studies. A study in 2007 by Lee et al[34] showed no effect on morbidity or mortality after elimination of routine UGI studies. UGI studies may not identify all leaks, and even among those identified, many patients do not require subsequent operation.[35–37] Serafini et al[38] demonstrated that UGI contrast studies detected three percent of leaks at the gastrojejunostomy anastamosis, which were subsequently managed conservatively by withholding oral intake until resolution of leak at repeat UGI 5 to 7 days later. This negates the routine use of postoperative Day 1 UGI studies unless clinical symptoms suggest concern for leak.
Carter et al[37] concluded that institutional inexperience and prolonged operative times were predictive of leaks using univariate analysis. Furthermore, postoperative UGI studies frequently show delayed of contrast material, suggestive of post-surgical edema, which is not clinically useful. Madan et al[32] concedes that with experience the leak rate has decreased. UGI studies may be of greater use among teaching centers to facilitate laparoscopic technical challenges, but as surgeons gain more experience, the PPV of UGI studies inevitably decreases, causing further questions regarding the usefulness of universal routine UGI studies on postoperative Day 1.
Disadvantages of UGI Studies
Questions of clinical management as well as increased pressure to reduce hospital length stay and cost of procedures has fueled the debate regarding the usefulness of UGI studies. The added cost varies dramatically from $75 to $750 per UGI study with radiology interpretation. Given the current number of procedures performed, routine UGI studies are approximated to cost six million dollars per year in the United States.[26,31] Furthermore, imaging of patients with obesity has equipment limitations and challenges of positioning, whereby proper intensifier placement, which can create scattered radiation and poor intra-abdominal visualization.[3] Patient discomfort, radiation exposure, risk of aspiration with swallowing of contrast, as well as a delay in diet initiation resulting in potentially longer hospital stays further provokes controversy. Currently the American Society for Metabolic and Bariatric Surgery (ASMBS) endorses the decision to perform routine versus selective UGI studies to be left to the discretion of the surgeon.[43]
Discussion
Adoption of new surgical techniques and technologies often comes with an innate concern for complications, which has validated the use of UGI studies for detection of leaks. A radiographic study with less-than-perfect sensitivity is not intended to rule out a condition; rather it should be used as a tool to support or negate clinical suspicion. Because UGI studies cannot appropriately evaluate the jejunojejunostomy anastamosis or biliopancreatic limb, the importance of clinical assessment, suspicion of leak, and judgment of the surgeon to proceed with operative management cannot be overemphasized.
The questions remain: Do negative UGI studies postoperatively give the surgeon or surgical team a false sense of security when a complication may exist? Or do UGI studies lead to postponement of diet and prolonged hospital stays and cost? Given the litigious atmosphere common in the United States, one can question whether the alleged cost of a diagnostic test to potentially assist in recognizing a potentially fatal condition earlier is well worth the inconvenience and expense. That cost cutting ought to occur outside the realm of increased confidence in patient management and care.
Conclusion
In the hands of experienced surgeons whose patients are clinically stable, UGI studies are not useful nor do they change management. UGI studies alone do not appropriately evaluate leaks, thus clinical assessment, suspicion of leak, and judgment of the surgeon to proceed with operative management cannot be over emphasized. Time should not be wasted performing an UGI study in the setting of true clinical concern. A prospective, randomized, controlled trial of routine versus selective UGI studies to detect leaks that evaluates the length of patient stay, hospital charges, patient discomfort, and confidence of changes in clinical decisions would be helpful to appropriately evaluate objective data of the safety and efficacy of UGI studies in post laparoscopic RYGB surgery.
References
1. Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults, 1999–2008. JAMA. 2010;303(3):235–241.
2. Center for Disease Control and Prevention (CDC). Behavioral risk Factor Surveillance system survey Data. Atlanta, Georgia: U.S. Department of Health and Human Services Center for Disease control and Prevention. http://www.cdc.gov/obesity/data/trends.html Accessed May 3, 2010
3. Merkle EM, Hallowell PT, Crouse C, Nakamoto DA, Stellato TA. Roux-en-Y gastric bypass for clinically severe obesity: Normal appearance and spectrum of complications at imaging. Radiology. 2005;234(3):674–683.
4. Livingston EH. Bariatric surgery in the new millennium. Arch Surg. 2007;142(10):919–922.
5. National Institutes of Health Analysis (NIH). 1991 Consensus Report. Bethesda, Maryland: U.S. Department of Health and Human Services. http://www.obesesurgery.com/NIH%20study.htm Accessed May 15, 2010
6. Ballantyne GH. Measuring outcomes following bariatric surgery: weight loss parameters, improvement in co-morbid conditions, change in quality of life and patient satisfaction. Obes Surg. 2003; 13(6): 954–964.
7. Omalu BI, Ives DG, Buhari AM, et al. Death rates and causes of death after bariatric surgery for pennsylvania residents, 1995 to 2004. Arch Surg. 2007;142(10):923–928.
8. The Longitudinal Assessment of Bariatric Surgery (LABS) Consortium. Perioperative safety in the longitudinal assessment of bariatric surgery. N Engl J Med. 2009;361(5):445–454.
9. Nguyen NT, Rivers R, Wolfe BM. Factors associated with operative outcomes in laparoscopic gastric bypass. J Am Coll Surg. 2003 10;197(4):548–555.
10. Lujan JA, Frutos MD, Hernandez Q, et al. Laparoscopic versus open gastric bypass in the treatment of morbid obesity: a randomized prospective study. Ann Surg. 2004 239: 433–437.
11. Anselmino M, Bammer T, Fernandez Cebrian JM, et al. Cost-effectiveness and budget impact of obesity surgery in patients with type 2 diabetes in three European countries(II). Obes Surg. 2009;19(11):1542–1549.
12. Campos GM, Ciovica R, Rogers SJ, et al. Spectrum and risk factors of complications after gastric bypass. Arch Surg. 2007;142(10):969–975.
13. Andres M, Perez M, Roldan J, et al. Roux-en-y gastric bypass: major complications. Abdom Imaging. 2007;32:613–618.
14. Carucci LR, Turner MA, Conklin RC, et al. Roux-en-Y gastric bypass surgery for morbid obesity: Evaluation of postoperative extraluminal leaks with upper gastrointestinal Series1. Radiology. 2006;238(1):119–127.
15. Scheirey CD, Scholz FJ, Shah PC, et al. Radiology of the laparoscopic roux-en-Y gastric bypass procedure: conceptualization and precise interpretation of results. Radiographics. 2006;26(5):1355–1371.
16. Varghese JC, Roy-Choudhury SH. Radiological imaging of the GI tract after bariatric surgery. Gastrointest Endosc. 2009;70(6):1176–1181.
17. Melinek J, Livingston E, Cortina G, Fishbein MC. Autopsy findings following gastric bypass surgery for morbid obesity. Arch Pathol Lab Med. 2002;126(9):1091–1095.
18. Almahmeed T, Gonzalez R, Nelson LG, et al. Morbidity of anastomotic leaks in patients undergoing Roux-en-Y gastric bypass. Arch Surg. 2007;142(10):954–957.
19. Bertucci W, White S, Yadegar J, et al. Routine postoperative upper gastroesophageal imaging is unnecessary after laparoscopic Roux-en-Y gastric bypass. Am Surg. 2006;72(10):862–864.
20. Dallal RM, Bailey L, Nahmias N. Back to basics: clinical diagnosis in bariatric surgery. routine drains and upper GI series are unnecessary. Surg Endosc. 2007;21(12):2268–2271.
21. Katasani VG, Leeth RR, Tishler DS, et al. Water-soluble upper GI based on clinical findings is reliable to detect anastomotic leaks after laparoscopic gastric bypass. Am Surg. 2005;71(11):916–918.
22. Mitchell MT. Bariatric imaging: Technical aspects and postoperative complications. Appl Radiol. 2008;37(2):10–22.
23. Gonzalez R, Nelson LG, Gallagher SF, Murr MM. Anastomotic leaks after laparoscopic gastric bypass. Obes Surg. 2004;14(10):1299–1307.
24. Fernandez AZ, DeMaria EJ, Tichansky DS, et al. Experience with over 3,000 open and laparoscopic bariatric procedures: multivariate analysis of factors related to elak and resultant mortality. Surg Endosc. 2004;18:193–197.
25. Sims TL, Mullican MA, Hamilton EC, et al. Routine upper gastrointestinal gastrografin swallow after laparoscopic roux-en-Y gastric bypass. Obes Surg. 2003;13(1):66–72.
26. Singh R, Fisher BL. Sensitivity and specificity of postoperative upper GI series following gastric bypass. Obes Surg. 2003;13(1):73–75.
27. Hamilton EC, Sims TL, Hamilton TT, et al. Clinical predictors of leak after laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Endosc. 2003;17(5):679–684.
28. Doraiswamy A, Rasmussen JJ, Pierce J, et al. The usefulness of routine postoperative upper GI series following laparoscopic gastric bypass. Surg Endosc. 2007;21(12):2159–2162.
29. Gonzalez R, Sarr MG, Smith CD, et al. Diagnosis and contemporary management of anastomotic leaks after gastric bypass for obesity. J Am Coll Surg. 2007;204(1):47–55.
30. Kolakowski S Jr, Kirkland ML, Schuricht AL. Routine postoperative upper gastrointestinal series after Roux-en-Y gastric bypass: Determination of whether it is necessary. Arch Surg. 2007;142(10):930–934.
31. White S, Han SH, Lewis C, et al. Selective approach to use of upper gastroesophageal imaging study after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2008;4(2):122–125.
32. Madan AK, Stoecklein HH, Ternovits CA, et al. Predictive value of upper gastrointestinal studies versus clinical signs for gastrointestinal leaks after laparoscopic gastric bypass. Surg Endosc. 2007;21(2):194–196.
33. DeMaria EJ, Sugerman HJ, Kellum JM, et al. Results of 281 consecutive total laparoscopic Roux-en-Y gastric bypasses to treat morbid obesity. Ann Surg. 2002;235(5):640–645.
34. Lee SD, Khouzam MN, Kellum JM, et al. Selective, versus routine, upper gastrointestinal series leads to equal morbidity and reduced hospital stay in laparoscopic gastric bypass patients. Surg Obes Relat Dis. 2007;3:413–416.
35. Bal B, Koch TR, Finelli FC, Sarr MG, Medscape. Managing medical and surgical disorders after divided Roux-en-Y gastric bypass surgery. Nat Rev Gastroenterol Hepatol. 2010;7(6):320–334.
36. Ballesta C, Berindoague R, Cabrera M, et al. Management of anastomotic leaks after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2008;18(6):623–630.
37. Carter JT, Tafreshian S, Campos GM, et al. Routine upper GI series after gastric bypass does not reliably identify anastomotic leaks or predict stricture formation. Surg Endosc. 2007;21(12):2172–2177.
38. Serafini F, Anderson W, Ghassemi P, et al. The usefulness of contrast studies and drains in the management of patients after Roux-en-Y gastric bypass. Obes Surg. 2002;12(1):34–38.
39. Fullum TM, Aluka KJ, Turner PL. Decreasing anastomotic and staple line leaks after laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2009:23:1403–1408.
40. Csendes A, Burdiles P, Burgos AM, et al. Conservative management of anastomotic leaks after 557 open gastric bypasses. Obes Surg. 2005;15(9):1252–1256.
41. Durak E, Inabnet WB, Schrope B, et al. Incidence and management of enteric leaks after gastric bypass for morbid obesity during a 10-year period. Surg Obes Relat Dis. 2008;4(3):389–393.
42. Frezza EE, Mammarappallil JG, Witt C, et al. Value of routine postoperative gastrographin contrast swallow studies after laparoscopic gastric banding. Arch Surg. 2009;144(8):766–769.
43. The ASMBS Clinical Issues Committee. ASMBS guideline on the prevention and detection of gastrointestinal leak after gastric bypass including the role of imaging and surgical exploration. Surg Obes Relat Dis. 2009;5(3):293–293.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}