
Anesthetic Concerns for Performing Bariatric Surgery in a Free-standing Ambulatory Center
by Jay B. Brodsky, MD, and Jerry Ingrande, MD
Dr. Brodsky is Professor (Anesthesia) and Medical Director: Perioperative Services, Stanford University Medical Center, Stanford, California. Dr. Ingrande is Instructor (Anesthesia) and Chief of Bariatric Anesthesia Division, Stanford University Medical Center.
Funding: There was no funding for the preparation of this manuscript.
Financial disclosure: The authors report no conflicts relevant to the content of this manuscript.
Bariatric Times. 2011;8(7):8–10
Abstract
More bariatric procedures are being performed on patients with morbid obesity in the outpatient setting. In this article, the authors review anesthetic considerations for the physician operating on outpatients with morbid obesity. The presence of comorbid conditions, such as obstructive sleep apnea and obesity hypoventilation, airway management, and anesthesia management plans are discussed.
Introduction
A major issue that remains unresolved among anesthesiologists and surgeons is whether or not patients with morbid obesity can safely undergo out-patient surgical procedures at free-standing ambulatory surgery facilities. Since these facilities often lack consultant physician and nursing back-up and support, specialized equipment, and the ability to care for a patient who may require an overnight stay or unplanned postoperative ventilation, there is reluctance among many anesthesiologists to accept any patient with morbid obesity as an outpatient. However, with increasing economic pressure to perform more complex surgery as outpatients, greater numbers of patients with obesity and morbid obesity are being considered for surgery[1] including bariatric procedures at free-standing facilities.[2]
Considerations in Performing Outpatient Surgery on the Patient Population with Morbid Obesity
BMI. Staff members at an outpatient facility often ask, “What is the maximum body mass index (BMI) acceptable for outpatient surgery?” Of course, BMI is not the most important factor. The presence of associated comorbidities and whether or not these conditions are medically controlled must first be considered. In addition, some surgical procedures may be safer than others for patients with obesity. Often the anesthetic management can be tailored for the individual patient with obesity to maximize safety.
Twenty years ago, when the current worldwide obesity epidemic was first recognized and at a time when free-standing outpatient surgical facilities were relatively new, the Royal College of Surgeons in the United Kingdom issued a document entitled “Guidelines for Day Case Surgery.” This document stated that any patient with a BMI of 30kg/m2 or more was unsuitable for operations performed as day-cases.[3] Without any evidence that obesity, per se, was a risk factor, their basis for choosing this arbitrary BMI remains unclear. Since this was only a guideline, many anesthesiologists and surgeons chose to simply ignore it. During the next decade, many reports appeared in the medical literature that documented an absence of significant differences in unplanned hospital admission rates or serious postoperative complications after day-case surgery in outpatients with BMIs of 35kg/m2 or more compared to patients with BMIs less than 25kg/m2.[4–6] Today, laparoscopic adjustable gastric banding (LAGB) procedures have been safely performed on patients with BMIs of 50kg/m2 or greater in the outpatient setting.
Obstructive sleep apnea. Without question the major concern for an anesthesiologist in determining whether a patient with morbid obesity is suitable or not for ambulatory surgery is the presence and degree of severity of obstructive sleep apnea (OSA). OSA is very common in patients obesity and in some series the incidence has been reported to be as high as 70 percent in bariatric patients.[7,8]
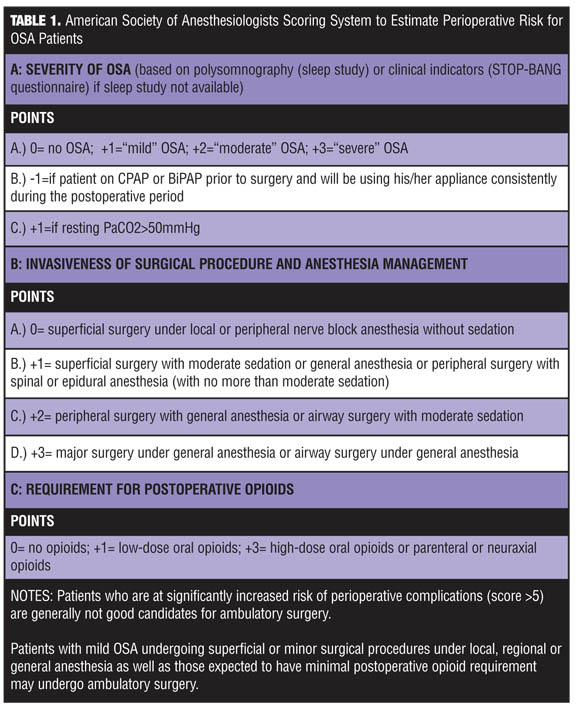
Diagnoses and risk assessment of OSA. The American Society of Anesthesiologists (ASA) published their own practice guidelines with a scoring system to predict whether a patient with OSA (normal-weight or obese) will be at an increased risk for perioperative complications.[9] Points are given based on the severity of the OSA, the degree of invasiveness of the planned operation, and whether or not the patient will need a general anesthetic and postoperative opioid analgesia (Table 1). A cumulative score is then calculated. The ASA recommended that patients with a score above five should not be considered candidates for ambulatory surgery. Since this system has not been clinically validated, it should only be used as a guide. Experience has demonstrated that patients with morbid obesity with mild or even moderate OSA, few if any co-existing medical comorbidities, well-controlled medical conditions, who will require minimal sedation or narcotic analgesia, and in whom a less invasive procedure is planned can successfully undergo outpatient surgery.
It is clear that OSA is frequently unrecognized and/or underdiagnosed. The patient may not even be aware that he or she snores, and simple observation of sleeping patterns by a partner is not always helpful in making the diagnosis. A definitive diagnosis of OSA and the degree of severity of the OSA can only be determined by a polysomnography (PSN) or “sleep study” at a sleep laboratory. A PSN study will confirm the presence of nocturnal sleep disturbances, including intermittent airway obstruction and the frequency of apnea (>10 second cessation of airflow despite continuous respiratory effort against a closed airway) and hypopnea events (50% reduction in airflow or a reduction associated with a decrease of oxygen saturation [SpO2]> 4%. Chronic OSA results in baseline hypoxemia and hypercapnia, pulmonary hypertension, and cardiac arrhythmias, all of which increase the risk of complications from anesthesia and surgery.
Unfortunately, sleep laboratories have different criteria for what constitutes “mild,” “moderate,” or “severe” OSA. For a variety of reasons, many patients (if not the majority) with obesity suspected of OSA will not have had a PSN study before their surgery. As an alternative, the STOP-BANG questionnaire, which evaluates snoring, tiredness during daytime, observed apnea, high blood pressure, body mass index (more than 35kg/m2), age (over 50 years), neck circumference (more than 40cm), and gender, can be used.[10] It contains eight simple questions (Table 2). If the patient answer yes to three or more of these questions, then a presumptive diagnosis of OSA can be made. The STOP-BANG questionnaire does not quantitate the severity of the OSA. Several of its criteria for OSA are almost always present in patients with morbid obesity, so it is our practice to consider and manage every patient with morbid obesity as if he or she has OSA. All older male bariatric surgical patients meet STOP-BANG criteria (i.e., high BMI, age >50 years, and male gender) for OSA.
Equipment. If a diagnosis of moderate-to-severe OSA is obtained by PSN, the patient should be fitted with a personal nasal continuous positive airway pressure (N-CPAP) device. The N-CPAP mask should be used for several weeks prior to scheduled elective surgery to normalize breathing during sleep. Patients who fail to respond to N-CPAP may do better with bi-level positive airway pressure (Bi-PAP), which combines pressure support ventilation and positive end-expiratory pressure (PEEP) via a nasal mask, that allows alveolar recruitment during inspiration and prevents alveolar collapse during expiration.
The potential benefit of N-CPAP or Bi-PAP for surgical patients with moderate-to-severe OSA appears to be great.[8] Although the majority of patients with morbid obesity probably have some degree of OSA, a N-CPAP mask will be prescribed and fitted only after a formal PSN study. Therefore, an argument can be made for testing all patients with morbid obesity scheduled for elective outpatient bariatric surgery and have N-CPAP started on those who can benefit from this intervention. Although a recent study11 of morbidity after ambulatory LAGB surgery found a relatively high incidence of transient postoperative hypoxemia (SpO2 <93%) in almost 40 percent of patients with a preoperative diagnosis of OSA, including those using N-CPAP, there were no instances of respiratory failure or need for re-intubation following surgery in any patient. The authors concluded that for patients at high risk for OSA, the significance of transient hypoxemia and the need to develop outpatient admission standards for patients with OSA still “remain to be determined” after LAGB.
Obesity hypoventilation syndrome. A small number of patients with morbid obesity have “obesity hypoventilation syndrome” (OHS), also called Pickwickian syndrome. OHS is characterized by hypersomnolence, right ventricular cardiac hypertrophy, pulmonary hypertension, polycythemia, hypervolemia, as well as hypoxemia and hypercapnia. Patients with OHS tend to be older, have super obesity, and have more restricted pulmonary function than the average patient with OSA. Hypoventilation is independent of intrinsic lung disease and is probably due to a progressive desensitization of the brain’s respiratory center to increased carbon dioxide from nocturnal sleep disturbances. Patients with OHS rely on a hypoxic ventilatory drive to breathe and they may hypoventilate or even stop breathing during emergence from general anesthesia when given oxygen. For those older patients with super obesity and a history of significant daytime somnolence, a preoperative arterial blood gas sample should be obtained with the patient breathing room air. If carbon dioxide retention is present, a diagnosis of OHS can be made. These patients should not be considered candidates for bariatric surgery at an ambulatory center since the risks of pulmonary complications requiring postoperative ventilatory assistance are very high in this population following general anesthetia. Whenever practical, a regional anesthetic should be used instead of general anesthesia for outpatients with obesity and OSA. Although individually, patients with obesity are more likely to have a failed block because of technical difficulties, as a group, when compared with normal-weight patients, postoperative pain, unanticipated hospital admissions, and overall patient satisfaction is similar after outpatient surgery under regional anesthesia. Unfortunately, regional anesthesia is not a feasible choice for bariatric surgery since laparoscopy requires a general anesthetic and tracheal intubation.
Airway management. Airway management in patients with morbid obesity, especially those with OSA, can be a challenge for the anesthesiologist, especially when he or she is alone and isolated in an ambulatory center. Supraglottic airway devices, such as the laryngeal mask airway (LMA), offer advantages over tracheal intubation and are particularly well suited for many outpatient operations. For example, in patients with moderate obesity (BMI 30–35kg/m2), an LMA can safely replace endotracheal intubation for peripheral operations.[12] Patients seem to tolerate the placement and maintenance of an LMA at a lower dose of anesthetic than needed for a tracheal tube, and muscle relaxants are not required for an LMA so problems with inadequate or incomplete neuromuscular after a short anesthetic are avoided. Unfortunately, an LMA is not an option for laparoscopy since it provides incomplete protection against aspiration of gastric contents, and the anesthesiologist may be unable to adequately deliver higher levels of positive pressure ventilation. Newer variants address both these limitations, and LMAs have been used instead of a tracheal tube during laparoscopy for selected gynecologic and general surgery procedures in patients with normal weight and obesity (BMI >30kg/m2). To date, there have been no published series reporting experience using an LMA for laparoscopic operations on patients with morbid obesity. Just because an LMA can be used does not mean it should be used if it compromises patient safety.[13] Current practice anesthetic standards require tracheal intubation for laparoscopic bariatric procedures.
A “difficulty airway” is often present in patients with morbid obesity, especially those with OSA. A difficult airway is defined as difficulty with face-mask ventilation, tracheal intubation, or both. Provision of adequate ventilation by face mask is often difficult in patients with obesity. Difficulties with tracheal intubation, although far less common, can occur even if the patient’s preoperative airway evaluation is normal. The head-elevated laryngoscopy position, in which the patient’s upper body, shoulders and head are “ramped” so that an imaginary horizontal line can be drawn from the sternum to the ear, will maximize view during direct laryngoscopy in patients with morbid obesity.[14]
Every facility where bariatric surgery is to be performed must have a “difficult airway cart” containing aides to intubation, such as a fiberoptic bronchoscope, a video-laryngoscope, bougies and airway exchange catheters, and a variety of LMAs. In addition, the anesthesiologist working with a patient with morbid obesity must always identify someone else with experience in airway management who can be nearby should problems occur during tracheal intubation and at the completion of the case following airway extubation. It is always risky to proceed with general anesthesia in patients with morbid obesity, whether in a stand-alone outpatient facility or in a regular operating theater, if an assistant who can help when needed is not readily available.
Anesthesia management. With today’s better understanding of the pharmacology of anesthetic drugs and techniques, anesthesia management plans can be modified to reduce complications in patients with obesity (Table 3). Minimizing or completely avoiding sedatives and opioids increases the safety of anesthesia for patients with morbid obesity. Inadequate or over-treatment of postoperative pain in the patient with morbid obesity will negatively impact postoperative recovery. Opioid-only analgesic regimens should be avoided because of their unacceptable respiratory-depressant side-effects in patients with morbid obesity. Balanced “multi-modal” analgesia combining regional or local analgesia when possible with nonopioid analgesic drugs, and giving opioids only in small amounts as rescue agents, is the best approach for treating postoperative pain. Intravenous (IV) infusions of either remifentanil or dexmedetomidine reduce the intraoperative use of opioids and decrease time spent in the postanesthesia care unit (PACU), in turn leading to earlier home discharge with fewer complications.[15,16]
Likewise, the occurrence of postoperative nausea (PN) with or without vomiting can prolong PACU stay or even lead to admission to a hospital. Generous amounts of IV fluids and multimodal prophylactic drug therapy with dexamethasone plus other agents will reduce the incidence and severity of PN, but cannot totally eliminate its occurrence.
Patient Discharge
Prior to discharge from the ambulatory surgical facility, the patient must be able to maintain his or her airway without any signs of obstruction. The patient’s oxygen saturation while breathing room air should return to baseline preoperative levels. Since postoperative complications can occur hours after surgery, especially in OSA patients, it is prudent to wait longer than usual before sending the patient home. The ASA guidelines recommend at least three hours of postoperative monitoring before discharging a patient with known OSA. Adherence to this protocol can restrict the ability to schedule patients with morbid obesity as outpatients, especially later in the day, since many facilities cannot stay open late to accommodate prolonged recovery room stays.
Comparison of Bariatric Procedures Performed in the Outpatient Setting
Recent reports of laparoscopic Roux-en-Y gastric bypass (RYGB) operations performed on outpatients have rekindled the debate of whether or not it is safe to perform bariatric surgery on patients with morbid obesity in an outpatient setting.[17] With careful patient selection, excluding patients with severe OSA or OHS and older patients with multiple medical comorbidities, even patients with super obesity have safely undergone outpatient LAGB operations at free-standing ambulatory surgery centers without serious complications.[18] However, for RYGB the situation is less clear. McCarty et al[19] reported a very large series of patients who underwent RYGB and were scheduled as outpatients. An impressive 84 percent of patients in the study required only a 23-hour stay before discharge. Since most ambulatory surgical facilities are not equipped for a 23-hour over-night stay, this experience may not be pertinent to the present discussion. More importantly, 14 percent of the study patients required admission to the hospital. This is a very high incidence for any outpatient procedure and would be unacceptable in a free-standing ambulatory surgery center.
Another single small study[20] reported one center’s experience in which increased BMI, along with advanced age and the presence of type 2 diabetes mellitus (T2DM) negatively affected same-day discharge after LAGB.
Conclusion
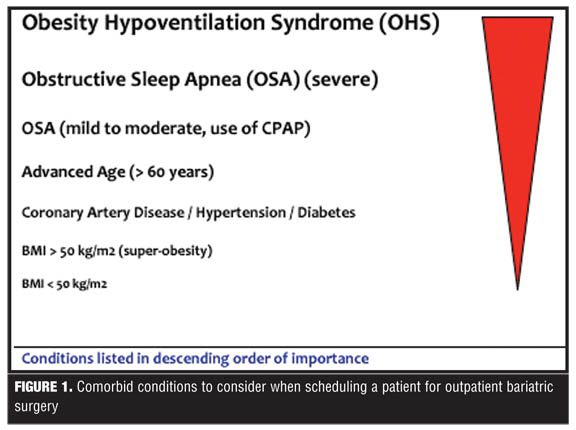
The increasing numbers of bariatric operations being performed, the expanding anesthetic and surgical experience with patients with morbid obesity undergoing procedures as outpatients, and advances in anesthetic techniques means that there will be increased pressure for more bariatric procedures to be performed on outpatients. However, there is now more overwhelming evidence that BMI itself should not be an indicator of suitability for outpatient surgery. From an anesthesiologist’s perspective, other factors, particularly the presence of OSA and not absolute weight itself, should determine who is an appropriate candidate for outpatient laparoscopic bariatric surgery (Figure 1).
References
1. Servin F. Ambulatory anesthesia for the obese patient. Curr Opin Anaesthesiol. 2006; 19:597–599.
2. Raeder J. Bariatric procedures as day/short stay surgery: is it possible and reasonable. Curr Opin Anaesthesiol. 2007;20:508–512.
3. Atkins M, White J, Ahmed K. Day surgery and body mass index: results of a national survey. Anaesthesia. 2002;57:180–182.
4. Davies KE, Houghton K, Montgomery JE. Obesity and day-case surgery. Anaesthesia. 2001;56:1112–1115.
5. Hofer RE, Kai T, Decker PA, Warner DO. Obesity as a risk factor for unanticipated admissions after ambulatory surgery. Mayo Clin Proc. 2008;83:908–916.
6. Bryson GL, Chung F, Cox RG, et al. Patient selection in ambulatory anesthesia—an evidence-based review: part II. Can J Anaesth.2004; 51:782–794.
7. Neligan PJ, Porter S, Max B, et al. Obstructive sleep apnea is not a risk factor for difficult intubation in morbidly obese patients. Anesth Analg. 2009;109:1182–1186.
8. Frey WC, Pilcher J. Obstructive sleep-related breathing disorders in patients evaluated for bariatric surgery. Obes Surg. 2003;13:676–683.
9. Gross JB, Bachenberg KL, Benumof JL, et al. American Society of Anesthesiologists Task Force on Perioperative Management. Practice guidelines for the perioperative management of patients with obstructive sleep apnea: a report by the American Society of Anesthesiologists Task Force on Perioperative Management of patients with obstructive sleep apnea. Anesthesiology. 2006;104:1081–1093.
10. Chung F, Elsaid H. Screening for obstructive sleep apnea before surgery: why is it important? Curr Opin Anaesthesiol. 2009;22:405–411.
11. Kurrek MM, Cobourn C, Wojtasik Z, et al. Morbidity in patients with or at high risk for obstructive sleep apnea after ambulatory laparoscopic gastric banding. Obes Surg. 2011;March 13 [Epub ahead of print]
12. Zoremba M, Aust H, Eberhart L, et al. Comparison between intubation and the laryngeal mask airway in moderately obese adults. Acta Anaesthesiol Scand. 2009;53:436–442.
13. Cooper RM. The LMA, laparoscopic surgery and the obese patient—can vs should. Can J Anaesth. 2003;50:5–10.
14. Collins JS, Lemmens HJ, Brodsky JB, et al. Laryngoscopy and morbid obesity: a comparison of the “sniff” and “ramped” positions. Obes Surg. 2004;14:1171–1175.
15. Song D, Whitten CW, White PF. Remifentanil infusion facilitates early recovery for obese outpatients undergoing laparoscopic cholecystectomy. Anesth Analg. 2000;90:1111–1113.
16. Paventi S, Santevecchi A, Perilli V, et al. Effects of remifentanil infusion bis-titrated on early recovery for obese outpatients undergoing laparoscopic cholecystectomy. Anesth Analg. 2006;102:1884–1898.
17. McCarty TM. Can bariatric surgery be done as an outpatient procedure? Adv Surg. 2006;40:99–106.
18. Montgomery KF, Watkins BM, Ahroni JH, et al. Outpatient laparoscopic adjustable gastric banding in super-obese patients. Obes Surg. 2007;17:711–716.
19. McCarty TM, Arnold DT, Lamont JP, et al. Optimizing outcomes in bariatric surgery. Outpatient laparoscopic gastric bypass. Ann Surg. 2005;242:494–501.
20. De Waele B, Lauwers MH, Massaad D, et al. Outpatient gastroplasty for morbid obesity: our first hundred cases. Obes Surg. 2010;20:1215–1218.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comments (2)
Trackback URL | Comments RSS Feed
Sites That Link to this Post