
Bariatric Surgery and Low Back Pain
This column is written by medical students and is dedicated to reviewing the science behind obesity and bariatric surgery.
Column Editor: Daniel B. Jones, MD, MS, FACS, FASMBS
Professor of Surgery, Harvard Medical School, Vice Chair, Beth Israel Deaconess Medical Center, Boston, Massachusetts
This month: Bariatric Surgery and Low Back Pain
by Victor D. Babatunde
Medical Student, Harvard Medical School, Boston, Massachusetts
ABSTRACT
Low back pain is a common health problem that is linked to obesity. Bariatric surgeries, such as vertical banded gastroplasty, adjustable gastric band, Rou-enx Y gastric bypass, and sleeve gastrectomy, are proven methods of weight loss. Recent studies have associated weight loss following bariatric surgeries with a significant decrease in disability and severity of low back pain. Further rigorous trials are needed to corroborate this increasing evidence that bariatric surgery may improve low back pain.
Bariatric Times. 2015;12(11):12–15.
Introduction
Low back pain (LBP) is a common health problem. Though, by itself, not a life threatening disease, it is a common cause of work-related disability and sickness absence.[1–3] Some of the common risk factors for LBP include psychosocial distress and cigarette smoking.[4,5] Obesity, in particular, has been linked to LBP and overall musculoskeletal (MSK) pain.[4,6,7] However, it is not well understood whether there is a causal relationship between the two.[8] It has been postulated that in obese patients, excess adipose tissue exerts additional mechanical pressure on weight bearing joints, such as the lumbar spine and knee, and may thus incite or worsen pain.[9] Bariatric surgeries, such as vertical banded gastroplasty (VBG), adjustable gastric band (AGB), Roux-en-Y gastric bypass (RYGB), and sleeve gastrectomy (SG), are proven methods of weight loss. Furthermore, such weight loss surgery (WLS) has been demonstrated to improve or resolve comorbid conditions of obesity, such as diabetes, hypertension, hyperlipidemia, gastroesophageal reflux disease (GERD), and nonalcoholic hepatic steatosis.[10] This article reviews the existing literature on the effects of WLS on LBP.
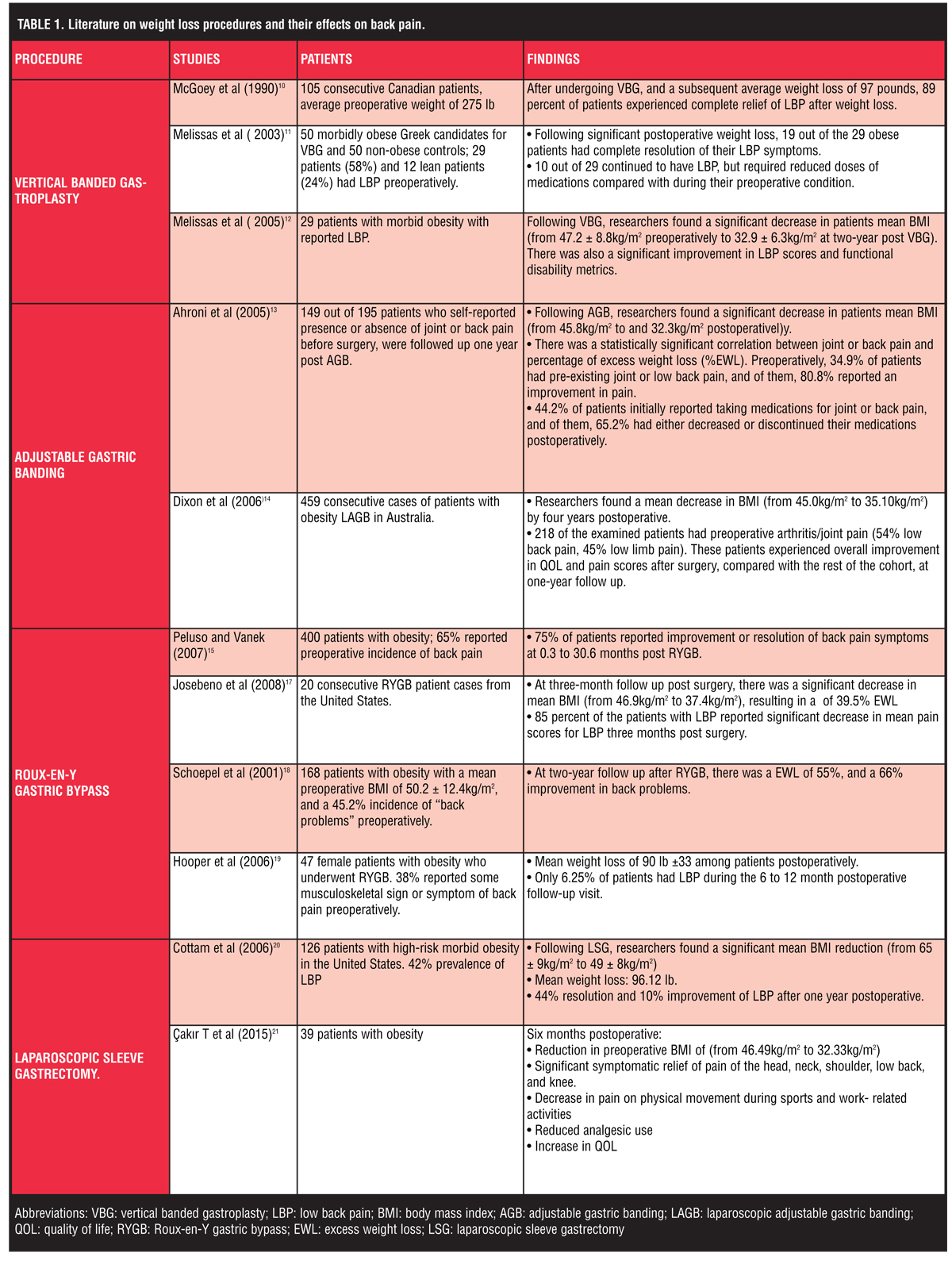
Weight loss procedures and their effects on back pain
Vertical banded gastroplasty. A number of studies have investigated the relationship between weight loss resulting from VGB and LBP. Of note, VGB is no longer commonly performed, as it has been replaced by other newer and more effective bariatric surgeries. As far back as 1990, McGoey et al,[9] in a case series that examined 105 consecutive Canadian patients with an average preoperative weight of 275 lb, and found that 88 percent of patients had activity limiting chronic MSK pain. Pain areas involved were documented by orthopedic surgeons using surveys and radiographs prior to operations, and included low back (62%), hips (11%), knees (57%), ankles (34%), and feet (21%). After undergoing VBG, and a subsequent average weight loss of 97 pounds, 89 percent of patients experienced complete relief of pain after weight loss. The McGoey study was later corroborated by a study performed by Melissas et al in 2003,[11] which examined 50 morbidly obese Greek candidates for VBG and 50 non-obese controls. Of these, 29 obese patients (58%) and 12 lean patients (24%) had LBP preoperatively.
Following significant postoperative weight loss, 19 out of the 29 obese patients had complete resolution of their LBP symptoms, while the remaining 10, who continued to have LBP, required reduced doses of medications compared with during their preoperative condition. They concluded that surgical weight reduction resulted in improvement and, in many cases, disappearance of LBP. In 2005, the same research group also examined 29 patients with morbid obesity with reported LBP.[12] Among these patients, there was a significant decrease in mean body mass index (BMI) from 47.2 ± 8.8kg/m2 preoperatively to 32.9 ± 6.3kg/m2 at two-year follow up post VBG. Along with weight loss, there was a significant improvement in LBP scores, and functional disability metrics.
Adjustable gastric banding. Several research groups have also examined AGB as a means for weight loss and reduction of LBP. In 2005, Ahroni et al[13] conducted a prospective study to examine the effects of laparoscopic AGB. One-hundred and forty-nine out of 195 patients who self-reported presence or absence of joint or back pain before surgery, were followed up one year post surgery. The mean BMI upon study entry was 45.8kg/m2, and 32.3kg/m2 postoperatively. There was a statistically significant correlation between joint or back pain and percentage of excess weight loss (%EWL). Preoperatively, 34.9 percent of patients had pre-existing joint or low back pain, and of them, 80.8 percent reported an improvement in pain. In addition, 44.2 percent of patients initially reported taking medications for joint or back pain, and of them, 65.2 percent had either decreased or discontinued their medications postoperatively.
In another study of AGB patients in 2006, Dixon et al[14] studied 459 consecutive cases of patients with obesity undergoing laparoscopic AGB (LAGB) in Australia. They found that there was a mean decrease in BMI from 45.0kg/m2 to 35.10 kg/m2 by four years after surgery. Two-hundred and eighteen of the examined patients had preoperative arthritis/joint pain (54% low back pain, 45% low limb pain). These patients experienced overall improvement in quality of life (QOL) and pain scores after surgery, compared with the rest of the cohort, at one-year follow up. It should be noted, however, that in this study, the percentage of excess weight loss at one year after surgery was not a major predictor in improved QOL.
Roux-en-Y gastric bypass. RYGB has also been investigated for its effect on LBP in a number of studies. In a 2007 retrospective study of 400 patients, Peluso and Vanek[15] examined the efficacy of RYGB surgery in the treatment of obesity-related comorbidities, including LBP. The preoperative incidence of back pain was 65 percent and, among these patients, 75 percent reported improvement or resolution of symptoms at 0.3 to 30.6 months post RYGB.
In 2009, Khoueir et al[16] explored the association between changes in BMI and clinical symptoms of axial LBP. In a longitudinal cohort of 58 patients who underwent bariatric surgery, 50 underwent RYGB, four had a duodenal switch gastric bypass, and four had SG. Of the 58 patients, 38 completed the entire study at 12 months postoperative. Of these patients, there was a mean decrease in BMI by 26.9 percent one year after surgery. LBP specific visual analog scale (VAS) scores were statistically significantly reduced by 44 percent from the preoperative to the postoperative setting. When these patients were examined one year after surgery, 68.4 percent of them improved in VAS scores, 13 percent remained stable, and 18.4 percent deteriorated. Overall, the Khoueir et al study suggests that substantial weight reduction after bariatric surgeries may be associated with moderate reductions in pre-existing back pain at early follow up.
In 2008, another study on RYGB examined 20 consecutive patient cases from the United States. Josebeno et al[17] found that at three-month follow up post surgery, there was a significant decrease in mean BMI from 46.9kg/m2 to 37.4kg/m2, resulting in a percent excess weight loss of 39.5%. For 85 percent of the patients with LBP, there was significant decrease in mean pain scores three months post surgery.
In 2001, Schoepel et al[18] examined 168 patients with obesity with a mean preoperative BMI of 50.2 ± 12.4kg/m2, and a 45.2 percent incidence of “back problems” preoperatively. At two-year follow up after RYGB, there was a percentage excess weight loss of 55%, and a 66 percent improvement in back problems. Another RYGB study by Hooper et al in 200619 examined 47 female patients with obesity who underwent RYGB. Of these patients, 38 percent had some musculoskeletal sign or symptom of back pain preoperatively. Patients showed a mean weight loss of 90 lb ±33 among patients. After weight loss, only 6.25 percent of patients had low back pain during the 6 to 12 month postoperative follow-up visit.
Laparoscopic sleeve gastrectomy. LSG is yet another weight loss surgery that has been associated with reduced LBP. In 2006, Cottam et al[20] conducted a prospective study of 126 patients with high-risk morbid obesity in the United States. The authors examined the efficacy of LSG (stage I) as an initial weight loss procedure and a subsequent RYGB (Stage II) on these patients. There was significant mean BMI reduction pre LSG to one year post SG (from 65 ± 9kg/m2 to 49 ± 8kg/m2, with a mean weight loss of 96.12 lb. Before SG, there was a 42-percent prevalence of LBP, and after SG, there was 44 percent resolution and 10 percent improvement of LBP after one year postoperative.
In a 2015 study examining the effects of laparoscopic LSG on head, neck, shoulder, lumbar spine, and knee pain in 39 patients with obesity, Cakir et al[21] found a reduction in preoperative BMI of 46.49kg/m2 to 32.33kg/m2 six months post surgery. As reported with pain scores compared to a preoperative baseline, there was a significant symptomatic relief of pain of the head, neck, shoulder, low back, and knee. There was also a decrease in pain on physical movement during sports and work- related activities, reduced analgesic use, and an increase in QOL after six months postoperative.
Multiple procedures. The different bariatric procedures have also been examined from a more collective viewpoint in relation to their effect on LBP. In 2012, Lidar et al,[22] studied 35 patients with morbid obesity who underwent bariatric surgery, including LAGB, LSG, laparoscopic RYGB, and duodenal switch. They examined the effect of weight loss on intervertebral disc space height, axial back pain (LBP), and radicular leg pain. They found a significant reduction in mean BMI from 42.8 ± 4.8kg/m2 pre surgery to 29.7 ± 3.4kg/m2 post surgery at one year follow up. Along with the significant increase in L4–L5 disc space height from 6 ± 1.3mm pre surgery to 8 ± 1.5 mm one year post surgery, there was a significant decrease in LBP and radicular leg pain. However, there was no association between the amount of weight reduction and the increment in disc space height or LBP improvement. Of note, prior reviews and studies in the literature show no direct link or correlation between degenerative magnetic resonance imaging (MRI) changes and development or duration of LBP.[23–25]
Another study by Hawkins et al[26] in 2007, examined 59 patients out of 79 consecutive series of patients who had undergone either laparoscopic RYGB or LAGB and completed follow up (median 14 months). They found a 32-percent increase in the number of respondents who were in paid work, and who experienced a significant increase in work productivity from 30.1 weekly work hours to 35.8 weekly work hours. In addition, significantly fewer patients claimed state benefits postoperatively.
Discussion
The majority of the research studies discussed here concluded that weight loss resulting from bariatric surgery is associated with significant improvement or, in certain instances, resolution of severity and disability associated with LBP. Further investigation of this exciting area is needed. Future research will need to address which bariatric surgical procedures, if any, are superior to others in relieving LBP. Moreso, questions remain as to how much weight loss correlates with reduction in LBP; is there a target BMI for patients before LBP improves significantly, and are there other factors, such as relief of other joint pain, in addition to weight loss, that correlate with relief of LBP? Orthopedic specialists and bariatric surgeons can both benefit from cross-disciplinary evidence-based use of bariatric surgery to address LBP and other joint pain, as this will seek to integrate understanding of physical functioning and QOL outcomes. Higher quality data collection and study comparison will be better achieved by minimizing variation in pain assessment through standardization of pain surveys, joint-specific pain-generating activities, and clinical examination tests.[27] Developing this research area will be important for generating refined evidence for setting expectations for bariatric patients.
See Table 1 for a summary of literature on weight loss procedures and their effects on back pain.
Acknowledgments: The author would like to thank Dr. Kevin McGuire for his insightful reviews and comments in the preparation of this article.
References
1. Brooks PM. The burden of musculoskeletal disease–a global perspective. Clin Rheumatol. 2006;25(6):778–781.
2. Andersson GB. Epidemiological features of chronic low-back pain. Lancet. 1999;354(9178):581–585.
3. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037.
4. Shiri R, Karppinen J, Leino-Arjas P, Solovieva S, Viikari-Juntura E. The association between obesity and low back pain: a meta-analysis. Am J Epidemiol. 2010;171(2):135–154.
5. Ramond A, Bouton C, Richard I, et al. Psychosocial risk factors for chronic low back pain in primary car—a systematic review. Fam Pract. 2011;28(1):12–21.
6. Deyo RA, Bass JE. Lifestyle and low-back pain. The influence of smoking and obesity. Spine (Phila Pa 1976). 1989;14(5):501–506.
7. Heuch I, Hagen K, Heuch I, Nygaard Ø, Zwart J-A. The impact of body mass index on the prevalence of low back pain: the HUNT study. Spine (Phila Pa 1976). 2010;35(7):764–768.
8. Garzillo MJ, Garzillo TA. Does obesity cause low back pain? J Manipulative Physiol Ther. 17(9):601–604.
9. McGoey B V, Deitel M, Saplys RJ, Kliman ME. Effect of weight loss on musculoskeletal pain in the morbidly obese. J Bone Joint Surg Br. 1990;72(2):322–323.
10. Maggard MA, Shugarman LR, Suttorp M, et al. Meta-analysis: surgical treatment of obesity. Ann Intern Med. 2005;142(7):547–559.
11. Melissas J, Volakakis E, Hadjipavlou A. Low-back pain in morbidly obese patients and the effect of weight loss following surgery. Obes Surg. 2003;13(3):389–393.
12. Melissas J, Kontakis G, Volakakis E, et al. The effect of surgical weight reduction on functional status in morbidly obese patients with low back pain. Obes Surg. 2005;15(3):378–381.
13. Ahroni JH, Montgomery KF, Watkins BM. Laparoscopic adjustable gastric banding: weight loss, co-morbidities, medication usage and quality of life at one year. Obes Surg. 2005;15(5):641–647.
14. Dixon JB, Dixon ME, O’Brien PE. Quality of life after lap-band placement: influence of time, weight loss, and comorbidities. Obes Res. 2001;9(11):713–721.
15. Peluso L, Vanek VW. Efficacy of gastric bypass in the treatment of obesity-related comorbidities. Nutr Clin Pract. 2007;22(1):22–28.
16. Khoueir P, Black MH, Crookes PF, et al. Prospective assessment of axial back pain symptoms before and after bariatric weight reduction surgery. Spine J. 2009;9(6):454–463.
17. Josbeno DA, Jakicic JM, Hergenroeder A, Eid GM. Physical activity and physical function changes in obese individuals after gastric bypass surgery. Surg Obes Relat Dis. 2010;6(4):361–366.
18. Schoepel KL, Olchowski SE, Mathis MW, Pridgen PD, Maxwell JG. Starting a successful bariatric surgical practice in the community hospital setting. Obes Surg. 2001;11(5):559-64.
19. Hooper MM. Tending to the musculoskeletal problems of obesity. Cleve Clin J Med. 2006;73(9):839–845.
20. Cottam D, Qureshi FG, Mattar SG, et al. Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity. Surg Endosc. 2006;20(6):859–863.
21. Çakır T, Oruç MT, Aslaner A, et al. The effects of laparoscopic sleeve gastrectomy on head, neck, shoulder, low back and knee pain of female patients. Int J Clin Exp Med. 2015;8(2):2668–2673.
22. Lidar Z, Behrbalk E, Regev GJ, et al. Intervertebral disc height changes after weight reduction in morbidly obese patients and its effect on quality of life and radicular and low back pain. Spine (Phila Pa 1976). 2012;37(23):1947–1952.
23. Chou D, Samartzis D, Bellabarba C, et al. Degenerative magnetic resonance imaging changes in patients with chronic low back pain: a systematic review. Spine (Phila Pa 1976). 2011;36(21 Suppl):S43–53.
24. Boden SD, Davis DO, Dina TS, Patronas NJ, Wiesel SW. Abnormal magnetic-resonance scans of the lumbar spine in asymptomatic subjects. A prospective investigation. J Bone Joint Surg Am. 1990;72(3):403–408.
25. Borenstein DG, O’Mara JW, Boden SD, et al. The value of magnetic resonance imaging of the lumbar spine to predict low-back pain in asymptomatic subjects: a seven-year follow-up study. J Bone Joint Surg Am. 2001;83-A(9):1306–1311.
26. Hawkins SC, Osborne A, Finlay IG, et al. Paid work increases and state benefit claims decrease after bariatric surgery. Obes Surg. 2007;17(4):434–437.
27. Vincent HK, Ben-David K, Cendan J, Vincent KR, Lamb KM, Stevenson A. Effects of bariatric surgery on joint pain: a review of emerging evidence. Surg Obes Relat Dis. 6(4):451–460.
FUNDING: No funding was provided.
FINANCIAL DISCLOSURES: The author reports no conflicts of interest relevant to the content of this article.
Category: Medical Student Notebook, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}