
Patient-reported Short-term Barriers to and Facilitators of Adherence to Behavioral Recommendations Following Bariatric Surgery
 by Aviva H. Ariel-Donges, PhD, MPH; Carlysa K. Oyama, BA; and Megan M. Hood, PhD
by Aviva H. Ariel-Donges, PhD, MPH; Carlysa K. Oyama, BA; and Megan M. Hood, PhD
Drs Ariel-Donges and Hood and Ms. Oyama are with the Department of Psychiatry and Behavioral Sciences, Rush University Medical Center.
FUNDING: No funding was provided.
DISCLOSURES: The authors have no conflicts of interest relevant to the content of this article.
ABSTRACT: Objective. The current study utilized a cross-sectional, nonrandomized design to evaluate patients’ understanding of their bariatric team’s postsurgical recommendations and to identify factors that facilitate or interfere with adherence to these recommendations.
Methods. Participants were recruited from an urban academic medical center’s bariatric psychology clinic. A total of 66 patients (83.3% female, 45.5% white, mean age=44.8±12.1 years, mean presurgical body mass index=46.99±7.27kg/m2, mean time postsurgery=10.0±6.0 months) completed a web-based assessment after undergoing either sleeve gastrectomy (66.7%) or Roux-en-Y gastric bypass (33.3%). A novel, seven-item self-report questionnaire measured patients’ understanding of their bariatric team’s recommendations, confidence in their ability to adhere to these recommendations, and experiences with potential barriers to and facilitators of adherence.
Results. Most participants reported “good” to “total” understanding of their physicians’ recommendations (>81.8%) and viewed all recommendations as being “important” to “very important” (>89.4%). The greatest proportion of participants (37.9%) endorsed exercise as the hardest recommendation to follow. Participants most commonly identified stress (39.4%) and needing to plan ahead (36.4%) as barriers to adherence. Seeing success at weight loss (86.4%), receiving support from family/friends (83.3%), and having other people notice their weight loss (78.8%) were seen as helpful for facilitating adherence to recommendations.
Conclusion. These findings indicate that patients who underwent bariatric surgery understood the major postsurgical behavioral recommendations and viewed these recommendations as valuable to their long-term outcomes. Exercise is a significant challenge for many, yet external sources of support and positive reinforcement might facilitate adherence.
KEYWORDS: Adherence, bariatric surgery, behavioral
Bariatric Times. 2020;17(7):15–17
Patient adherence is a significant factor in long-term weight-loss outcomes following bariatric surgery.1,2 To promote long-term weight loss and prevent medical complications, patients undergoing bariatric surgery are instructed to adhere to four main areas of postsurgical behavioral recommendations: 1) follow specific eating and drinking behaviors; 2) exercise regularly; 3) take medication/supplements daily; and 4) attend follow-up medical appointments. However, adherence to these guidelines is generally poor.3
Key bariatric dietary recommendations include eating three meals per day, consuming primarily lean protein (>60g per day) and nonstarchy vegetables, and avoiding high-fat or high-sugar foods and drinks.4 Up to 52 percent of patients report poor adherence to dietary guidelines after surgery,3,5–9 and there is evidence to suggest that depressive symptoms, preference for sweets, and prior disordered eating predict worse dietary adherence.3,7,10–13
Frequent engagement in physical activity (>150 minutes per week)4 is one of the strongest predictors of postoperative weight loss,2,13–16 yet it’s one of the least followed recommendations.2,17,18 Approximately 50 to 70 percent of patients report nonadherence to physical activity recommendations.2,5,7,10,13,14,19 Lack of time, low motivation, and health issues (e.g., chronic pain, poor stamina) have been cited as common barriers to high levels of physical activity both before and after surgery.20
Taking supplements (e.g., iron, calcium, vitamin D, and vitamin B12) on a daily basis is a key behavioral recommendation to prevent postsurgical nutritional deficiencies.4 Some studies indicate that rates of adherence to taking vitamins start high,9,19,21,22 while others suggest that vitamin adherence is poor even immediately postsurgery.5,8,23,24 Studies consistently report that adherence declines in the years following surgery, with up to 54 to 67 percent of patients reporting vitamin nonadherence at longer-term follow-up.8,16,21,25,26
Finally, 45 to 89 percent of patients fail to attend medical appointments in the years after surgery, which is concerning given that appointment attendance is correlated with long-term weight-loss outcomes.7,27–32 Evidence suggests lower rates of attendance for younger patients, unemployed patients, and patients with a lower presurgical body mass index (BMI).1-3,31
Successful adherence requires both understanding of the behavioral recommendations and the ability to overcome barriers to implementing those behaviors in everyday life.33 While a number of studies assess rates of adherence postsurgery, few assess perceived barriers and very few assess perceived facilitators to adherence. Research on motivational interviewing and self-determination theory indicate that knowledge about, perceived importance of, and self-confidence for engaging in a potential behavior change impacts individuals’ ultimate ability to sustain new health behaviors.34 Accordingly, the current study attempted to further expand understanding of potential barriers and facilitators to adherence by asking postsurgery patients to assess how well they felt they understood the recommendations that were given to them, how important they felt these recommendations were to their success, and how confident they were that they could adhere to the recommendations.
The current study is important because it aimed to fill a gap in the literature by a) evaluating patients’ perceived understanding of their bariatric team’s recommendations, b) obtaining patients’ views of the importance of these recommendations, c) assessing patients’ confidence in their ability to adhere to these recommendations, and d) identifying factors that patients feel either facilitate or interfere with adherence following surgery. Given how difficult it is to engage patients in postoperative programs for improving adherence,3,35–37 proactively identifying factors that might lead to poor adherence, as well as factors that support adherence efforts, is vital to developing effective, individualized interventions during the preoperative phase. By better understanding these factors experienced by patients undergoing bariatric surgery, clinicians can more efficiently provide resources to overcome common barriers and encourage use of existing facilitators to maximize patient adherence and surgery outcomes.
Methods
Design. The study utilized a cross-sectional, nonrandomized design to assess barriers to and facilitators of adherence to postsurgical behavioral recommendations. Any individual who was seen by the bariatric psychology team between 2015 and 2017, underwent bariatric surgery, and provided an email address was eligible for the study. Surveys were emailed to 269 individuals on three occasions around a single time point regardless of patients’ surgery date, and 24.5 percent (N=66) responded to the invitation to participate in the study. Participants were compensated $10. Weight data was collected retrospectively at a later date from patients’ medical records. Descriptive statistics were utilized to present participant characteristics and responses. Qualitative responses to open-ended questions about additional patient-identified barriers and facilitators were also reported. Pearson correlations were used to assess relationships between responses and weight outcomes (percent excess weight loss and BMI change) at 12 months postsurgery, with significance cut-off set at p=0.001 to correct for multiple correlations.
Setting. Participants were recruited from a bariatric psychology clinic within an urban academic medical center in the Midwest. This study was approved by the academic medical center’s Institutional Review Board.
Participants. A total of 66 participants (83.3% female, mean age=44.8 ±12.1 years, mean presurgical BMI=46.99±7.27kg/m2) completed the assessment after undergoing bariatric surgery. Participants were mostly white (45.5%) or black/African American (34.8%); 9.1 percent identified as multiracial, and 10.6 percent did not report their race. Most participants (72.7%) did not identify as Hispanic/Latino. Participants had undergone sleeve gastrectomy (66.7%) or Roux-en-Y gastric bypass (33.3%). Mean time since surgery at the time of the assessment was 10.0±6.0 months (range=1 to 30 months); 77.3 percent of the sample (n=51) was at least six months post-surgery, and 47.0 percent of the sample (n=31) was between 6 to 12 months postsurgery. Weight change data at 12 months postsurgery, which was collected retrospectively for the purposes of this study, was available for 83.3 percent of participants (n=55). Average weight change at 12 months postsurgery was -12.02±4.90kg/m2 or -58.52±25.31 percent of excess body weight. Two participants (3.0%) did not provide responses to all questions.
Measurements. The study utilized a novel, seven-item self-report assessment of patients’ perceived understanding of their team’s recommendations, understanding of the team’s rationale for the recommendations, views of the importance of these recommendations, and confidence in their ability to adhere to these recommendations, as well as ratings of a variety of potential barriers to and facilitators of adherence. Responses were rated on 5-point Likert scales ranging from 1 (anchors depending on the item: do not understand at all, not at all confident, not at all a barrier, or not at all helpful) to 5 (total understanding, very confident, very significant barrier, or very helpful). The assessment also included space for optional, free-text descriptions of patient-identified barriers and facilitators that were not listed in the survey.
Results
The majority of participants reported “good” to “total” understanding of their team’s recommendations for eating/drinking (90.9%), exercise (84.9%), medication/vitamins (84.5%), and attending medical appointments (81.8%). Only 3.0 percent of participants reported “poor” understanding of one or more of these recommendations, and only one participant (1.5%) reported that they did “not understand at all” one of the recommendations (appointment attendance). Almost all participants further reported “good” to “total” understanding of why their team made recommendations for eating/drinking (87.9%), exercise (89.4%), medication/vitamins (89.4%), and appointments (89.4%). Almost no participants (0–1.5%) reported “poor” understanding of why these recommendations were made, and none reported that they “did not understand at all.” Most participants also viewed recommendations as being “important” to “very important” for eating/drinking (92.4%), exercise (90.9%), medication/vitamins (92.4%), and appointments (89.4%). Across these categories, 0 to 3.0 percent of participants reported their team’s recommendations were “not important,” and only one participant (1.5%) reported that recommendations for attending medical appointments were “not at all important.”
Most participants reported being “confident” or “very confident” in their ability to adhere to recommendations for eating/drinking (77.3%), exercise (62.1%), medication/vitamins (74.2%), and appointments (77.3%). Only 4.6 to 7.6 percent reported being “not confident” or “not at all confident” about their ability to adhere to these recommendations.
Exercise recommendations were identified as the hardest to follow after surgery by the greatest percentage of participants (37.9%), followed by dietary intake (25.8%), taking medications/vitamins (24.2%), and attending medical appointments (9.1%).
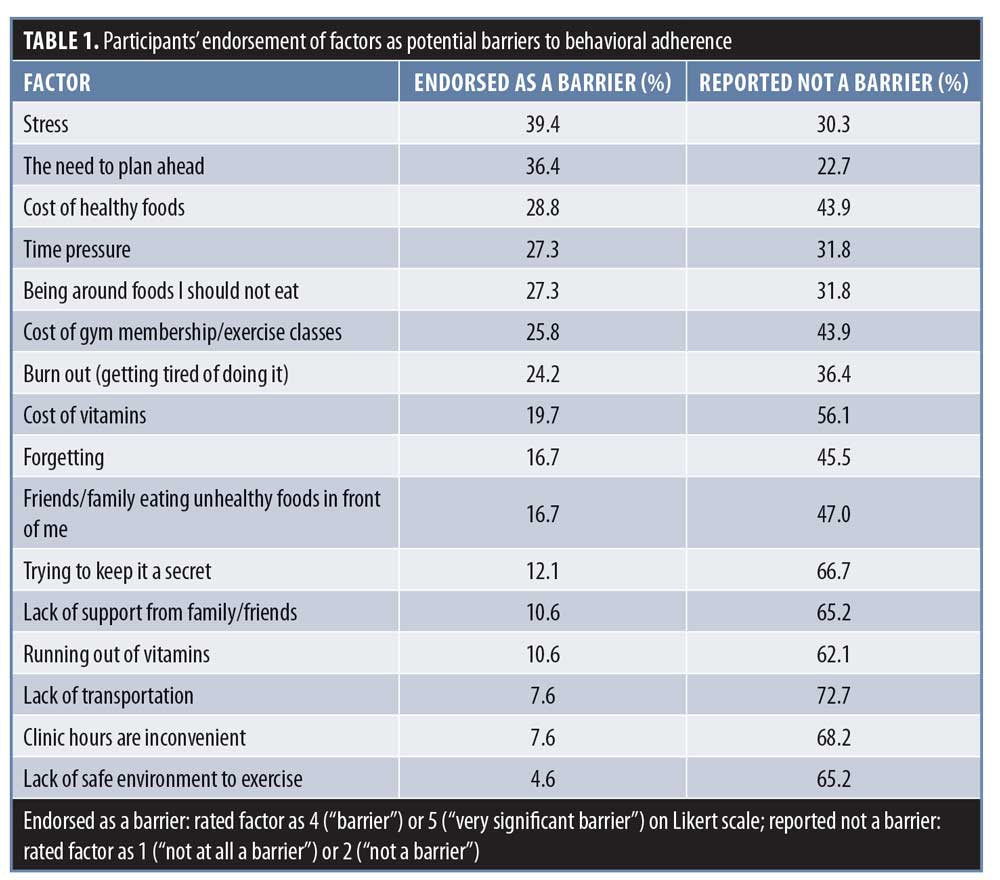
The greatest number of participants identified stress and needing to plan ahead as “barriers” or “very significant barriers” to adherence. The fewest number of participants endorsed lack of transportation, inconvenient clinic hours, and lack of safe exercising environment as barriers to adherence (Table 1). Twenty-two participants (33.3%) provided free-text responses about additional barriers, and the greatest proportion (31.8%) reported having physical barriers to engaging in exercise (e.g., lack of energy, damaged spinal nerves, arthritis, and pain and stiffness). Other free-text responses identified difficulties changing lifelong habits, unrelated medical complications, disliking taking pills, inconvenient work schedules, and postsurgical depressive symptoms as barriers to following recommendations.
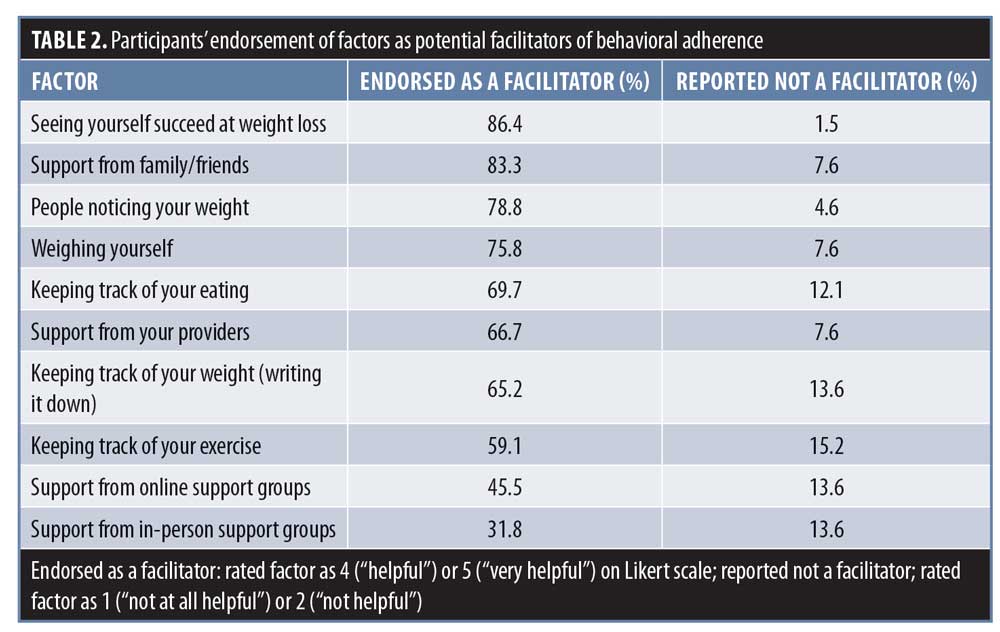
The greatest number of participants identified seeing success at weight loss, receiving support from family/friends, and having other people notice their weight loss as “helpful” or “very helpful” for adherence to recommendations. The fewest number of participants identified support from online and in-person support groups as facilitators of adherence (Table 2). Four participants (6.1%) provided free-text responses about additional facilitators not included in the questionnaire. These responses identified the importance of a positive environment, encouraging self-talk, online resources, and purchasing smaller clothing as facilitators of adherence.
Time since surgery was not associated with participants’ understanding of their team’s recommendations (ps>0.23), understanding of why their team made recommendations (ps>0.09), belief that their team’s recommendations were important (ps>0.03), confidence in their ability to adhere to recommendations (ps>0.003), or self-reported barriers to (ps>0.09) or facilitators of (ps>0.12) adherence. Similarly, postoperative weight change was not associated with participants’ understanding of their team’s recommendations (ps>0.41), understanding of why their team made recommendations (ps>0.51), belief that their team’s recommendations were important (ps>0.46), confidence in their ability to adhere to recommendations (ps>0.007), or self-reported barriers to or facilitators of adherence (ps>0.02).
Discussion
Patients who underwent bariatric surgery reported excellent understanding of their team’s recommendations, viewed these recommendations as important for their success, and largely felt confident in their ability to adhere. Regularly engaging in behaviors that are complex and have a high risk of leading to “behavioral fatigue” require internal motivation.38 Understanding what the recommended behaviors are, why they are important, and feeling confident in one’s ability to perform the behaviors is key for developing this internal drive.34,39 The results of the present study are highly encouraging given that patients who underwent bariatric surgery reported high levels of these internal resources, which might help motivate them to use creative problem solving for external barriers to sustained adherence.
Notably, there was significant variability in ratings of barriers and facilitators, which highlights how obstacles and support mechanisms might differentially impact patients. Although higher levels of physical activity are strongly associated with greater long-term weight loss, this study replicated prior findings that exercising is often viewed as the most difficult behavior to follow.2,14–15,40 Adherence to dietary recommendations emerged as the second largest patient-identified challenge, which is also consistent with prior studies.6,41–42 Current findings suggest that many patients view support mechanisms, such as receiving positive feedback from others and seeing one’s weight-loss success, as factors that enhance their ability to adhere to postoperative recommendations. Stress and the need to plan ahead were identified as primary obstacles to adherence.
Tailored postsurgical programs might be needed to help each patient maximize adherence, yet current findings suggest that enhancing patients’ sense of support and providing encouraging feedback might benefit the majority. Providers themselves can be a source of support, and prior research indicates that strong patient–provider relationships and frequent follow-up contacts can have a positive impact on outcomes.43 Creative strategies that account for both barriers and facilitators to change might be particularly useful, such as employing telemedicine visits and mobile health technologies that increase the availability of support for patients while reducing transportation barriers.44,45 Finally, given the difficulties many patients report in trying to adhere to exercise recommendations and the importance of regular exercise for long-term weight-loss maintenance, bariatric surgery programs should consider providing structured support specifically for physical activity.46–48
Weight change at 12 months postsurgery was not associated with understanding of behavioral recommendations, confidence in one’s ability to adhere to recommendations, or self-reported barriers to or facilitators of adherence. Given the strong influence of metabolic changes over the first 12 months postsurgery,2,3,5,15 behavioral adherence was not expected to affect the shorter-term weight-change outcomes explored in the present study. Future studies should examine these relationships at longer-term follow-up periods.
Limitations. Strengths of the present study include a literature-based assessment, minimal missing data, and broad inclusion criteria. It should be noted, however, that these findings are based upon an urban, largely female population in the Midwest and might not be reflective of all patients who undergo bariatric surgery. One limitation of survey studies is the possibility of selection bias; therefore, future studies should aim to assess the study constructs in a wider sample of postsurgery patients to determine the generalizability of these results. Due to the cross-sectional nature of the survey, time since surgery ranged widely for participants but did not appear to relate to patients’ responses in the current study. Additionally, mean time since surgery was brief (10±6.0 months), so participant responses are likely not representative of long-term adherence factors. Experiences of barriers and facilitators might change over time, and future studies would benefit from assessing these factors at multiple time points in the same participants after surgery.49 While the present study utilized self-reported data—the most commonly used measure in bariatric research49—future studies using objective measures of behavioral adherence (e.g., actigraphy, dietary recall, and electronically monitored supplement adherence) might provide more specific details on adherence behaviors. Previous research suggests that self-report typically overestimates adherence,50–52 so self-reported “total” understanding of behavioral recommendations in the present study, for example, should not be equated with objectively accurate understanding of recommendations. Finally, given the novelty of this area of research and the relatively small sample size, data analyses were limited to descriptive statistics and correlations.
The authors hope that the preliminary data in the present study will spur additional research that is adequately powered to allow for more detailed statistical analysis of the relationships among the variables studied.
Conclusion
The present study provides insight into patients’ perspectives after bariatric surgery, including challenges patients experience related to behavioral adherence. Following recommendations for postsurgical dietary choices and engaging in regular physical activity are important for long-term weight-loss outcomes. Patients most commonly reported that stress and needing to plan ahead were barriers to their adherence, while experiencing initial weight loss and receiving social support were valuable facilitators of maintaining healthy behaviors after surgery. Further research is warranted to explore 1) objective patient understanding of the bariatric team’s behavioral recommendations; 2) whether perceived barriers and facilitators are associated with actual rates of adherence; 3) what factors moderate perceptions of barriers and facilitators; and 4) whether self-identified barriers and facilitators of adherence predict long-term weight change.
References
- Karmali S, Brar B, Shi X, et al. Weight recidivism post-bariatric surgery: a systematic review. Obes Surg. 2013;23:1922–1933.
- Yanos BR, Saules KK, Schuh LM, Sogg S. Predictors of lowest weight and long-term weight regain among Roux-en-Y gastric bypass patients. Obes Surg. 2015;25:1364–1370.
- Hood MM, Corsica J, Bradley L, et al. Managing severe obesity: understanding and improving treatment adherence in bariatric surgery. J Behav Med. 2016;39:1092–1103.
- Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient–2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endo Pract. 2013;19:
337–372. - Dagan SS, Keidar A, Raziel A, et al. Do bariatric patients follow dietary and lifestyle recommendations during the first postoperative year? Obes Surg. 2017;27:
2258–2271. - Thomas JG, Bond DS, Ryder BA, et al. Ecological momentary assessment of recommended postoperative eating and activity behaviors. Surg Obes Relat Dis. 2011;7:206–212.
- Toussi R, Fujioka K, Coleman KJ. Pre‐and postsurgery behavioral compliance, patient health, and postbariatric surgical weight loss. Obesity. 2009;17:996–1002.
- Schiavo L, Scalera G, Pilone V, et al. Patient adherence in following a prescribed diet and micronutrient supplements after laparoscopic sleeve gastrectomy: our experience during 1 year of follow‐up. J Human Nutr Diet. 2017;30:98–104.
- Wnuk S, Azim B, Sockalingam S. Behavioral and psychosocial predictors of adherence to dietary recommendations one-year post-bariatric surgery. Surg Obes Relat Dis. 2019;15:S100.
- Elkins G, Whitfield P, Marcus J, et al. Noncompliance with behavioral recommendations following bariatric surgery. Obes Surg. 2005;15:546–551.
- Gorin AA, Raftopoulos I. Effect of mood and eating disorders on the short-term outcome of laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2009;19:1685–1690.
- Sarwer DB, Wadden TA, Moore RH, et al. Pre-operative eating behavior, post-operative dietary adherence, and weight loss after gastric bypass surgery. Surg Obes Relat Dis. 2008;4:640–646.
- Welch G, Wesolowski C, Piepul B, et al. Physical activity predicts weight loss following gastric bypass surgery: findings from a support group survey. Obes Surg. 2008;18:517–524.
- Herman KM, Carver TE, Christou NV, Andersen RE. Keeping the weight off: physical activity, sitting time, and weight loss maintenance in bariatric surgery patients 2 to 16 years postsurgery. Obes Surg. 2014;24:1064–1072.
- Sheets CS, Peat CM, Berg KC, et al. Post-operative psychosocial predictors of outcome in bariatric surgery. Obes Surg. 2015;25:330–345.
- Welch G, Wesolowski C, Zagarins S, et al. Evaluation of clinical outcomes for gastric bypass surgery: results from a comprehensive follow-up study. Obes Surg. 2011;21:18.
- Bond DS, Jakicic JM, Unick JM, et al. Pre- to postoperative physical activity changes in bariatric surgery patients: self report vs. objective measures. Obesity. 2010;18:2395–2397.
- El Chaar M, McDeavitt K, Richardson S, et al. Does patient compliance with preoperative bariatric office visits affect post-operative excess weight loss? Surg Obes Relat Dis. 2011;7:743–748.
- Lier HO, Biringer E, Stubhaug B, Tangen T. The impact of pre-operative counseling on post-operative treatment adherence in bariatric surgery patients: a randomized controlled trial. Patient Educ Couns. 2012;87:336–342.
- Peacock JC, Sloan SS, Cripps B. A qualitative analysis of bariatric patients’ post-surgical barriers to exercise. Obes Surg. 2014;24:
292–298. - Cooper PL, Brearley LK, Jamieson AC, Ball MJ. Nutritional consequences of modified vertical gastroplasty in obese subjects. Int J Obes. 1999;23:382–388.
- James H, Lorentz P, Collazo-Clavell ML. Patient-reported adherence to empiric vitamin/mineral supplementation and related nutrient deficiencies after Roux-en-Y gastric bypass. Obes Surg. 2016;26:2661–2666.
- Nadkarni A, Domeisen N, Hill D, Fernandez A. Patient adherence to vitamin therapy following bariatric surgery. Surg Obes Relat Dis. 2016;12:S199.
- Zarshenas N, Tapsell LC, Neale EP, et al. The relationship between bariatric surgery and diet quality: a systematic review. Obes Surg. 2020;15:1–25.
- Sunil S, Santiago VA, Gougeon L, et al. Predictors of vitamin adherence after bariatric surgery. Obes Surg. 2017;27:416–423.
- Mahawar KK, Clare K, O’Kane M, et al. Patient perspectives on adherence with micronutrient supplementation after bariatric surgery. Obes Surg. 2019;29:1551–1556.
- Elrefai M, Hasenberg T, Vassilev G, Otto M. Adherence to a follow-up program is improving weight loss. Bari Surg Pract Pat Care. 2017;12:173–177.
- Garb J, Welch G, Zagarins S, et al. Bariatric surgery for the treatment of morbid obesity: a meta-analysis of weight loss outcomes for laparoscopic adjustable gastric banding and laparoscopic gastric bypass. Obes Surg. 2009;19:1447–1455.
- Goldenshluger A, Elazary R, Cohen MJ, et al. Predictors for adherence to multidisciplinary follow-up care after sleeve gastrectomy. Obes Surg. 2018;28:3054–3061.
- Higa K, Ho T, Tercero F, et al. Laparoscopic roux-en-Y gastric bypass: 10-year follow-up. Surg Obes Relat Dis. 2011;7:516–525.
- Larjani S, Spivak I, Guo MH, et al. Preoperative predictors of adherence to multidisciplinary follow-up care postbariatric surgery. Surg Obes Relat Dis. 2016;12:350–356.
- Martens K, Pester B, Hecht L, et al. Adherence to health care appointments is associated with weight loss following bariatric surgery. Surg Obes Relat Dis. 2019;15:S174.
- O’Leary A. Self-efficacy and health. Behav Res Ther. 1985;23:437–451.
- Patrick H, Williams GC. Self-determination theory: its application to health behavior and complementarity with motivational interviewing. Int J Behav Nutr Phys Act. 2012;9:18.
- Kalarchian MA, Marcus MD, Courcoulas AP, et al. Optimizing long-term weight control after bariatric surgery: a pilot study. Surg Obes Relat Dis. 2012;8:710–716.
- Lent MR, Campbell LK, Kelly MC, et al. The feasibility of a behavioral group intervention after weight-loss surgery: a randomized pilot trial. PloS One. 2019;14:1–15.
- Sarwer DB, Moore RH, Spitzer JC, et al. A pilot study investigating the efficacy of post-operative dietary counseling to improve outcomes after bariatric surgery. Surg Obes Relat Dis. 2012;8:561–568.
- Bray GA, Wadden TA. Improving long‐term weight loss maintenance: can we do it? Obesity. 2015;23:2–3.
- Ng JY, Ntoumanis N, Thøgersen-Ntoumani C, et al. Self-determination theory applied to health contexts: a meta-analysis. Persp Psych Sci. 2012;7:325–340.
- Egberts K, Brown WA, Brennan L, O’Brien PE. Does exercise improve weight loss after bariatric surgery? A systematic review. Obes Surg. 2012;22:335–341.
- Bradley LE, Sarwer DB, Forman EM, et al. A survey of bariatric surgery patients’ interest in post-operative interventions. Obes Surg. 2016;26:332–338.
- Shah M, Simha V, Garg A. Long-term impact of bariatric surgery on body weight, comorbidities, and nutritional status. J Clin Endo Metab. 2006;91:4223–4231.
- Gourash WF, Ebel F, Lancaster K, et al. Longitudinal Assessment of Bariatric Surgery (LABS): retention strategy and results at 24 months. Surg Obes Relat Dis. 2013;9:514–519.
- Huang JW, Lin YY, Wu NY. The effectiveness of telemedicine on body mass index: a systematic review and meta-analysis. J Telemed Telecare. 2018;25:389–401.
- Livhits M, Mercado C, Yermilov I, et al. Is social support associated with greater weight loss after bariatric surgery? A systematic review. Obes Rev. 2011;12:142–148.
- Coen PM, Goodpaster BH. A role for exercise after bariatric surgery? Diab Obes Metab. 2016;18:16–23.
- Coleman KJ, Caparosa SL, Nichols JF, et al. Understanding the capacity for exercise in post-bariatric patients. Obes Surg. 2017;27:51–58.
- Zagarins SE, Allen NA, Skinner SS, et al. Improved exercise behaviors associated with a comprehensive structured exercise program following bariatric surgery. Bari Nurs Surg Pat Care. 2011;6:85–90.
- Hood MM, Kelly MC, Feig EH, et al. Measurement of adherence in bariatric surgery: a systematic review. Surg Obes Relat Dis. 2018;14:1192–1201.
- Bond DS, Jakicic JM, Vithiananthan S, et al. Objective quantification of physical activity in bariatric surgery candidates and normal weight controls. Surg Obes Relat Dis. 2010;6:72–78.
- King WC, Hsu JY, Belle SH, et al. Pre- to postoperative changes in physical activity: report from the longitudinal assessment of bariatric surgery-2. Surg Obes Relat Dis. 2012;8:522–535.
- Modi AC, Zeller MH, Xanthakos SA, et al. Adherence to vitamin supplementation following adolescent bariatric surgery. Obesity. 2013;21:E190–195.
Category: Original Research, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.


