
Can Iron Alone Sharpen Iron? Managing Iron Deficiency in the Bariatric Surgery Patient
by Jennifer Traub, RD, CNSC
Author Affiliation: Ms. Traub is a Clinical Dietitian at Hurley Bariatric Center, Flint, Michigan.
Funding: No funding was provided for the preparation of this article.
Financial Disclosure: Ms. Traub reports no conflicts of interest relevant to the content of this article.
Bariatric Times. 2010;7(12):24–26
Abstract
Properly diagnosing and finding an effective way to correct an iron deficiency that occurs after bariatric surgery can be somewhat perplexing to many healthcare providers. Useful laboratory parameters and assessment of clinical symptoms, as well as treatment options, are discussed.
Introduction
While there are many challenges in maintaining optimum health status in patients who have undergone bariatric surgery, one issue that remains puzzling for many healthcare professionals is accurately diagnosing and treating iron deficiency. Iron deficiency can present with or without anemia, and its overall incidence is high in the bariatric surgery patient population. Proper diagnosis and management is essential in relieving patient symptoms and preventing long-term consequences associated with iron deficiency, such as impaired memory, physical ability, and mental function.
Bariatric surgery patients are at an increased risk of iron deficiency. The incidence of anemia following bariatric surgery has been reported to be as high as 74 percent and has been mostly ascribed to iron deficiency.[2] There are three major factors that contribute to the increased risk in this patient population. First, surgical bypass procedures reduce absorptive surface area by the exclusion of the duodenum and proximal jejunum, which are the physiological sites of iron absorption. Second, the newly formed gastric pouch has a reduced capacity and is hypoacidic, which reduces the bioavailability of oral iron as well as the function of iron transport molecules.
Third, dietary sources of heme iron, a form of iron easily absorbed by the body, such as red meat, tend to be poorly tolerated by many patients after having bariatric surgery and, therefore, the oral intake of these dietary sources of iron is reduced.[3]
Iron deficiency without anemia
A normal hemoglobin (Hgb) level does not automatically mean a person is not iron deficient. Patients with normal body iron stores have to lose a significant portion of those stores before their Hgb level alone indicates that iron deficiency is present (Hgb<12g/dL for women or Hgb<13g/dL for men). Therefore, assessment of clinical symptoms (chronic fatigue is the most prevalent) as well as use of other biochemical screening tools are necessary to effectively identify iron deficiency in the absence of a decreased Hgb level. For example, normal Hgb with a low (or in the low end of normal range) mean corpuscular hemoglobin (MCH) or elevated red cell distribution width (RDW) point to mild iron deficiency without anemia. Further assessment of ferritin levels (<30ng/mL) in the absence of inflammation (C-reactive protein <0.5mg/dL) or normal ferritin levels with low transferrin saturation (<20%) if inflammation is present can serve as the main laboratory diagnostic tools for iron deficiency.[1]
Iron deficiency with anemia
Iron deficiency with anemia will appear much like the description of iron deficiency without anemia with low transferrin saturation percentages and low ferritin concentrations in the absence of inflammation; however, low Hgb levels (Hgb<12g/dL for women or <13g/dL for men) will also exist. Because mean corpuscular volume (MCV) is a late indicator in patients without active bleeding, a low MCH is a better red-cell marker for detecting iron deficiency in circulating red blood cells in an otherwise stable post-bariatric surgery patient. It is also important to note that coexisting macrocytic (e.g., B12 or folate) deficiencies may mask microcytosis in those patients who are indeed iron deficient.[1] Therefore, testing of those B12 and folate levels is crucial prior to determining an appropriate treatment path.
Treatment options
Once a deficiency in iron stores has been diagnosed, treatment is often a confusing matter. Oral iron supplements usually comprise of one of three iron salts: iron sulfate, iron gluconate, and iron fumarate. Oral iron can be given as tablets or elixirs. In tablets, there are nonenteric-coated and enteric-coated pills and extended-release formulas. Extended-release and enteric-coated iron supplements are generally better tolerated (gastrointestinally) than nonenteric-coated tablets but they tend to contain less bioavailable iron and may not be absorbed at all due to a resected duodenum in many bariatric surgery patients.[4] Therefore, an initial recommendation of nonenteric-coated tablets and assessing for gastrointestinal (GI) intolerance, such as nausea, epigastric discomfort, and constipation, are prudent.
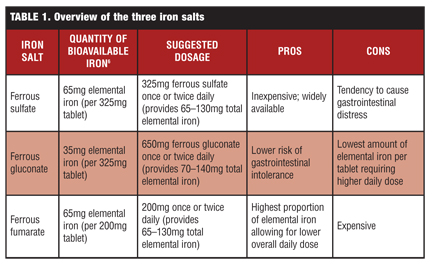
Ferrous sulfate is the least expensive and most commonly used of the available over-the-counter (OTC) oral iron supplements.[6] However, it tends to cause GI distress and is not as effectively absorbed as ferrous fumarate, as the fumarate salt contains more bioavailable iron than the sulfate salt. Ferrous gluconate contains the least amount of elemental iron of the three ferrous salts, making it the least recommended form of oral iron supplementation.[8] As a result, ferrous fumarate is preferred over either ferrous sulfate or ferrous gluconate in terms of efficacy. Yet, ferrous fumarate is generally more expensive than ferrous sulfate, and can be cost prohibitive for many patients. Table 1 provides an overview of the three iron salts. It should also be noted that because iron can be poisonous, there are polysaccharide iron complexes available that have lower levels of toxicity as well as improved rates of tolerance from a GI standpoint, but such formulations decrease the availability of absorbable iron, making them less than ideal when trying to manage a known iron deficiency in a patient population that is already at an increased risk for deficiency.[1,7]
A low level of acidity in the GI tract can greatly affect iron absorption in the post-bariatric surgery patient. Therefore, patients should not take iron supplements within two hours of taking antacids. To further complicate matters, certain medications, such as proton pump inhibitors and H2 blockers, which are routinely prescribed after bariatric surgery, can further impair iron absorption. Additionally, because calcium, phosphorus, and magnesium salts impair the absorption of elemental iron and happen to be a common ingredient in most multivitamin preparations, multivitamins alone should never be recommended as a sole therapy for a known iron deficiency.[4] Given our knowledge about how the pH level of the GI tract affects iron absorption, we can use this information to help optimize treatment for our patients. It is well documented that the use of ascorbic acid, or vitamin C, increases the bioavailability of oral iron supplements[.4,5] Hence, the routine recommendation of vitamin C in conjunction with iron supplementation can improve the overall effectiveness of oral iron therapy.
Effective treatment for identified iron deficiency may be accomplished with 65 to 130mg of elemental iron one to two times per day (each 325mg tablet of ferrous sulfate and 200mg tablet of ferrous fumarate provides approximately 65mg elemental iron, respectively). If iron parameters do not improve within several months of starting oral therapy, the dosage may need to be increased. Menstruating women may require up to six tablets per day to correct a known iron deficiency.[9]
For those patients who self discontinue oral iron therapy due to the GI side effects that often accompany a commonly recommended dose of 150 to 200mg of daily elemental iron, changing the type of iron salt and formulation as well as dose reduction, which often requires a lengthening of the dose interval, may allow iron-intolerant patients to continue with their oral iron therapy.[4]
Given that the most effective forms of OTC elemental iron supplements (i.e., ferrous fumarate) can be costly for some patients, a prescription iron supplement, which sometimes proves to be a more effective form of treatment for similar or less cost, can be offered to patients. There are available prescription iron supplements that contain both elemental iron as well as vitamin C to optimize absorption. Additionally, because of the critical role cobalamine and folate play in hematopoiesis, many prescription iron preparations also contain vitamin B12 and folate, further improving the usefulness of the overall therapy (e.g., Ferrex 28 and Multigen Plus, Breckenridge Pharmaceuticals, Boca Raton, Florida).
Refractory iron deficiency
Not all patients with iron deficiency respond to oral supplementation, whether OTC or prescription. This can be especially common in patients who have an altered GI tract. It has been documented that patients with severe forms of iron deficiency anemia (Hgb <10g/dL) do not respond to oral treatment alone. Individuals who have shown to be refractory to oral iron supplementation, whether due to the severity of their deficiency or because of GI intolerance, may need parenteral/intravenous iron treatment that does not rely on intestinal absorption.[9] Such patients should be referred to a hematologist for management of their anemia.
Conclusion
In managing a post-bariatric surgery patient with a clearly identified iron deficiency, initial replacement of 65 to 130mg of elemental iron once or twice per day (preferably in the form of ferrous fumarate due to its higher content of elemental iron) in conjunction with >60mg vitamin C is appropriate. Given the risk of macrocytic deficiency as well as the metabolic requirements of normal hematopoiesis, it is important to monitor vitamin B12 and folate levels to ensure they are adequate, correcting as indicated. If biochemical iron parameters do not return to normal limits within a few months of treatment commencement, one of the prescription iron replacement formulations may prove effective. Once again, the physician should recheck laboratory parameters within a few months. If the patient’s iron deficiency does not respond to oral therapy attempts, the patient should be referred for parenteral iron therapy.
References
1. Muñoz M, Botella-Romero F, Gómez-Ramírez S, et al. Iron deficiency and anaemia in bariatric surgical patients: causes, diagnosis and proper management. Nutr Hosp. 2009;24(6):640–654.
2. von Drygalski A, Andris DA. Anemia after bariatric surgery: more than just iron deficiency. Nutr Clin Pract. 2009;24,2:217–226.
3. Ruz M, Carrasco F, Rojas P, et al. Iron absorption and iron status are reduced after Roux-en-Y gasatric bypass. Am J Clin Nutr. 2009;90:527–532.
4. Alleyne M, Horne MK, Miller JL. Individualized treatment for iron-deficiency anemia in adults. Am J Med. 2008;121:943–948.
5. Marinella MA. Anemia following Roux-en-Y surgery for morbid obesity: A review. South Med J. 2008;101(10):1024–1031.
6. National Anemia Action Council. A Physician’s Guide to Oral Iron Supplements. http://www.anemia.org/
professionals/feature-articles/content.php?contentid=306§ionid=15. Accessed November 29, 2010.
7. McDiarmid, Johnson. Are any oral iron formulations better tolerated than ferrous sulfate? J Fam Pract. 2002;51(6):576.
8. National Institutes of Health. Office of Dietary Supplements. Dietary Supplement Fact Sheet: Iron. http://ods.od.nih.gov/factsheets/ironAccessed November 29, 2010.
9. Love AL, Billett HH. Obesity, bariatric surgery, and iron deficiency: true, true, true and related. Am J Hematol. 2008;83:403–409.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
Nice content but slow search processing