
Early Complications of 120 Laparoscopic Greater Curvature Plication Procedures
by Youssef Andraos, MD; Dany Ziade, MD; Rana Achcouty, MD; and Mariette Awad, PhD
Dr. Andraos is Chief, Department of Bariatric Surgery, Abou Jaoude Hospital, Beirut, Lebanon; Dr. Ziade is Chief, Department of Anesthesiology, Abou Jaoude Hospital, Beirut, Lebanon; Dr. Achcouty is an anesthesiologist, Abou Jaoude Hospital, Beirut, Lebanon; and Professor Awad is Assistant Professor, Electrical and Computer Engineering Department, American University of Beirut (AUB), Beirut, LebanonFunding: No funding was provided for the preparation of this article.
Financial disclosure: The authors report no conflicts of interest relevant to the content of this article.
Bariatric Times. 2011;8(9):10–15
Abstract
Reduction of gastric volume is traditionally the primary mechanism by which patients can lose weight safely. Weight loss is made possible by different procedures, including sleeve gastrectomy, vertical banding gastroplasty, and perigastric ring. Since the success rate of these procedures is variable and the complications associated with them are severe, laparoscopic greater curvature plication is emerging as an alternative, safe option for reduction of the gastric volume. In this case series, the authors discuss the first 120 cases performed at Hospital Abou Jaoude, Beirut, Lebanon, since December 2010. The initial results as well as early complications and management are discussed.
Introduction
A number of bariatric surgical procedures achieve weight loss in patients by multiple mechanisms, including restriction of food intake. Adjustable gastric banding (AGB) and vertical sleeve gastrectomy (VSG) are restrictive procedures that reduce the volume of ingested food in a patient. Roux-en-Y gastric bypass (RYGB) and duodenal switch (DS) work by diminishing the quantity of and the absorption of ingested food.[1,2,5,6,15] AGB, VSG, RYGB, and DS can all be highly effective in achieving weight loss; however, they are not without significant complications, such as perforation, slippage, and gastric erosions for bands. Moreover, VSG, DS, and RYGB are irreversible procedures and are associated with high rates of perforation, bleeding, infection due to foreign material in the body, and gastric leaks.[3,4,7,13–15] Leaks in a patient who has undergone VSG are dangerous and can lead to morbidity and mortality. Leaks after VSG are difficult to manage, especially at the level of Angle of His.
Complications in AGB, VSG, RYGB, and DS are due to negative pressure in the subphrenic region (continuous aspiration), high intragastric lumen pressure, stenosis, and obstruction of the gastric tube, all of which can lead to reoperation and may even cause death.[15–18] This case series highlights the early complications of laparoscopic greater curvature plication (LGCP), a new restrictive bariatric surgical technique. LGCP reduces the size of the stomach without the use of an implant or gastric resection, unlike other bariatric procedures.
Methods
The present case series was conducted using the National Institute of Health’s (NIH)1 inclusion criteria for bariatric surgery. This criteria states that patients with a body mass index (BMI) of 40kg/m2 or more, or a BMI of over 35kg/m2 with at least one comorbidity, can benefit from weight reduction via gastric restrictive surgeries. United States Food and Drug Administration (FDA) approval of AGB performed with the Lap-Band (Allergan, Irvine, California) in patients with a BMI of 40kg/m2 or more or a BMI of 30kg/m2 or more and one or more obesity-related comorbid conditions was also included selection of patients for surgery.[2] All patients underwent a multidisciplinary evaluation by an endocrinologist, cardiologist, psychologist, nutritionist, and pneumologist, as well as blood and barium meal tests. The case series also received the approval of the local ethics committee at Abou Jaoude Hospital in Beirut, Lebanon.
From December 2010 to June 2011, a total of 120 patients underwent LGCP. This case series included 40 men and 80 women, with a mean age of 36 years (range 18–58 years) and mean BMI 40.4kg/m2 (range 30–63kg/m2).
All complications were monitored and recorded intraoperatively through to the end of the first month. The anesthesiologist and the Committee of Morbidity at Abou Jaoude Hospital monitored all patients postoperatively.
Technique
Positioning. A standard position on the operative table was adopted for all patients. Patients were placed under general anesthesia in an anti-Trendlenburg position at 30-degree French position (operator between legs) and two assistants one each side of the patient.
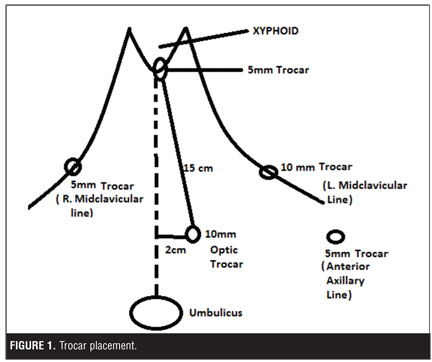
A five-trocar port technique was used for all patients except for those with a small left liver for whom a four-trocar technique was adopted (Figure 1). The operation began with an 18mmHg pneumoperitoneum, which was created at the palmer’s point on the upper left quadrant. The first trocar of 10mm was placed 15cm from the xiphoid process and 2cm left to the midline for the 30-degree laparoscope. A second 10mm trocar was inserted at the upper left quadrant on the midclavicular line. A third 5mm trocar was inserted on the left flank at the anterior axillary line. A fourth 5mm trocar was inserted at the xiphoid process on the left of the hepatic falciform ligament. Finally, a fifth 5mm trocar was inserted in the upper right quadrant at the midclavicular line.
We began the procedure by lifting the left liver lobe and fixing it by a grasp (EndoCinch,™ Davol, A Bard Company, Warwick, Rhode Island) attached to the anterior part of the left crus. Then, the greater sac was entered by dissecting the greater curvature between the gastric body and the antrum at the horizontal branch of the crow’s feet.
The posterior gastric wall was held up and the body of the stomach was freed from posterior attachment, the gastrosplenic short vessels, the omentum (without the necessity to dissect the left crus), and the angle of His. The same maneuver was achieved on the greater curvature vessels distally, and stopped 3cm before the pylorus. Posterior gastric adhesions near the lesser curvature were not dissected to prevent the distortion of the new stomach. Gastric plication was created by the invagination of the greater curvature over a 32 French tube.
It is important to note that the first point of the first row must be imbricated to fix the whole fundus in order to prevent fold invagination and intraesophagal fold migration. For this purpose, a total gastric point was made.
The first row was stopped 3cm before the pylorus. In the second row, we used nonabsorbable 2/0 thread, which fixed the first row and gave the final shape and volume of the imbricated stomach. The distance between each point was 2 to 3cm from the great curvature anteriorly and posteriorly in the first and the second row with the midline fixed at each point.
Additional separated stitches were used in some cases when the distance between stitches was larger than 2cm. This was performed in order to prevent fold herniation between stitches. In four reoperation cases (two operations following band removal and two operations following vertical banding gastrectomy), the gastric tissue was thicker and additional separated stitches were used The final aspect of the stomach was shaped like a small J as in SG procedures, slightly larger but full from the inside and fixed (Figure 2).
At the end of the operation, the gastric tube was removed. Leak and patent lumen tests were performed in all cases with 50 to 100mL of diluted methylene blue. Hemostasis was verified at the end of all operations. The anesthesiologist verified that patients’ blood pressure before exuflation was above the pneumoperitoneum pressure, which was decreased to 10mm of mercury. Trocars were removed from the abdominal wall but kept inserted in the subcutaneous fat. If no bleeding occurred, the residual pneumoperitonium was aspirated and no drain was placed at the end of the operation. Six hours postoperatively, the patients were asked to walk.
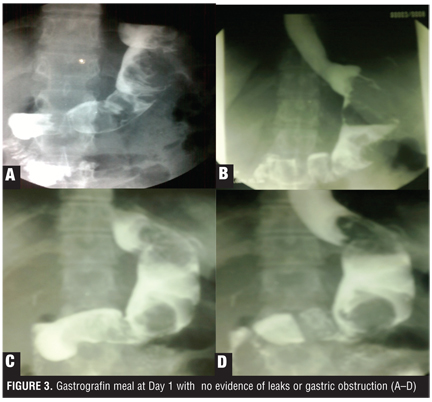
At Postoperative Day 1, patients were given gastrografin meal. If no obstruction or leaks were noticed, the patients were discharged from the hospital. Liquid was given to all patients immediately after the gastrografin meal at a rate of one teaspoon each 20 minutes and as tolerated. If no vomiting occured, the patient was discharged from hospital with a prescription of proton pump inhibitor (PPI) single dose for two months; antispasmodic and antiemetic suppositories, if needed; and chewable multivitamins for the first 10 days postoperatively. Figure 3 shows the gastrografin meal at Postoperative Day 1 with no evidence of leaks or gastric obstruction.
The postoperative diet was prescribed by the dietitian based on clear liquids for the first week and semi-liquids as tolerated for three weeks. Patients were allowed solid food four weeks postoperatively. Follow-up visits for the assessment of safety and weight loss were scheduled postoperative at two weeks, one month, three months, six months, 12 months, 18 months, and 24 months.
Complications and Management in the Case Presented
Intraoperative complications. Bleeding. Bleeding was the major intraoperative complication in our series. Hemostasis was achieved in all cases without the need of blood transfusion. No postoperative reoperation was needed for hemoperitoneum. The following different bleeding cases occurred:
1. One case was converted into laparotomy for mesentric trocar lesion and massive bleeding (trocar blade defect with no major vessel lesion). Hemoperitoneum was aspirated (1000mL), mesentery was sutured, and gastric plication was achieved by laparotomy (Figure 4).
2. Two cases of left hepatic subcapsular hematoma occurred and were managed conservatively with complete resorption at one month postoperatively.
3. Two cases of gastrosplenic vessel bleeding (300mL) occurred and hemostasis was achieved intraoperatively by clips and catherization.
4. One case of moderate mesocolic bleeding (500mL) controlled by laparoscopy was observed and plication was achieved as planned (Figure 5). Three cases of massive trocar port bleeding (200mL) were observed. Bleeding control was achieved by reverdin needle suturing. Minor trocar port bleeding (50mL) was controlled by monopolar coagulation.
6. Three cases of intramural gastric parietal hematoma were observed and managed by compression.
7. One case of severe subcutaneous emphysema related to a pneumomediastinum occurred when hiatal hernia cure was associated to LGCP, (operation was achieved at low intra-abdominal pressure).
8. No cases of injuries of adjacent organs (spleen, pancreas, small bowel or colon) was noted.
Early postoperative complications. We refer to early postoperative complications as any complication that occurred during the Postoperative Month 1. No bleeding occurred. The main complications observed were obstruction and leak.
Obstruction. Intraesophageal fold invagination. One case of obstruction in the intraesophegeal fold invagination occurred Figure 6). This complication is specific to LGCP and occurred in a patient when the fundus plication was not fixed.
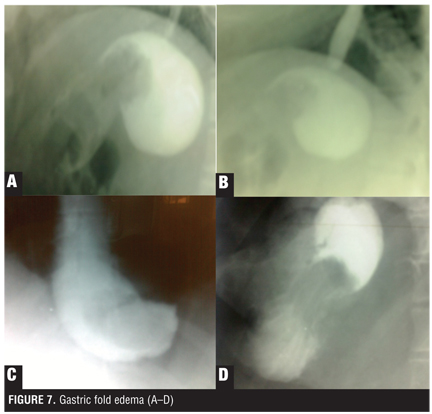
Gastric fold edema. Gastric fold edema is a complication specific to LGCP (Figure 7). We observed one case of complete gastric obstruction by edema of the fold plication. The patient required reoperation (a looser plication) at Day 3. This patient also developed a perisplenic abscess with no evidence of gastric fistula. The abscess was treated with intravenous (IV) antibiotics for three weeks with no need of percutaneous drainage).
Five cases of fold edema with complete obstruction of the residual gastric lumen were noticed on Postoperative Day 1 at the gastrografin meal control. Spontaneous resolution was achieved after four days in two cases, five days in two cases, and seven days for one case. These patients were kept at the hospital on IV line fluid administration and electrolytes. Moderate hypocalcaemia was also noted in these five cases and was treated by IV calcium gluconate. In 2007, Talebpour and Amoli concluded that fold edema is mainly due to venous stasis and operative trauma.[10]
We obeserved two cases of food intolerance with no evidence of obstruction on gastrografin meal. The food intolerance in these patients resolved immediately after gastroscopy at Postoperative Day 10 (gastrografin meal control was normal at Postoperative Day 1).
Fold rupture and fold herniation. Fold rupture and herniation are complications specific to LGCP. We observed one case of fold rupture and herniation in our case series. In this patient, the upper part of the first row of the plication was broken and a large gastric pouch was formed, leading to a complete obstruction and gastric leak (Figure 8).
Leaks. One case of gastric fistula was observed at Postoperative Day 3 (Figures 9a–9c), 3cm below the gastroesophageal (GE) junction of the anterior face of the stomach with generalized peritonitis (Figure 9e). The plication was removed laparoscopically and suturing of the leak hole (Figure 9d) was made by absorbable thread. A looser plication (Figure 9f) was performed at the same time. The patient was kept on IV antibiotics for three weeks and nasogastric tube was left for three days postoperatively.
Minor complications. No major complications (i.e., death, blood clots) were observed in our group of patients. Some minor complications occurred incuding minor hematemesis in seven cases and melena in two cases. These complications were managed conservatively with PPI at high doses.
We observed one case of transitory brachial paralysis, which regressed within 72 hours, and one case of left pneumonia, which resolved after five days of IV antibiotics.
Late complications. We refer to late complications as any complications observed in the patient up to six months postoperatively. Only two cases in our series developed late complications. One case of spontaneous hemoperitonium occurred six weeks after LGCP. The investigation showed corpus luteum rupture, which was treated conservatively by two units of blood transfusion. Spontaneous resorption was achieved within 15 days and monitored by magnetic resonance imaging (MRI). One case of upper gastric bleeding two months after operation by fold ulceration was observed and treated by gastroscopy and adrenaline injection with the transfusion of two units of blood.
Results
One-hundred and twenty patients underwent LGCP over a period of six months at Abou Jaoude Hospital. The mean operative time was 65 minutes (ranges: 45–90) and the mean hospital stay was 36 hours. Among the treated patients, 112 patients (93.3 %) left the hospital after 24 hours, six patients (5%) were kept more than one day due to fold edema, and one patient (0.8%) was kept more than one day due to gastric leak. One case of gastric plication was done by laparotomy (conversion) and the patient was dismissed from the hospital on Postopertive Day 4.
All of the observed intraoperative complications did not change our strategy to accomplish the gastric greater curvature plication. The majority of our intraoperative complications were related to laparoscopy (trocar lesion, trocar port bleeding, pneumomediastinum), and were not specific to greater curvature plication.
Specific early complications were mainly due to the complete obstruction of the residual gastric pouch by fold edema (5%), extrinsic compression by intramural gastric hematoma (2%), or elastic gastric effect of suturing and gastric tube distortion (0.8%).
Severe early complications, notably the only case (0.8%) of gastric obstruction, were managed rapidly in our early experience by reoperation. If complete obstruction was seen after a gastrografin meal on Postopertive Day 1 with patent intraoperative methylene blue test, patients were kept on IV fluid for 3 to 5 days. Fold edema decreased progressively without need for any other treatment or re-intervention.
Peritonitis, which occurred in one patient on Postoperative Day 3 from gastric leak, was managed laparoscopically by suturing the leak hole and cleaning the whole peritoneum cavity. Two drains were left; a looser plication was performed. Antibiotics were given for three weeks and the patient lost 25 percent of excess weight one month postoperatively.
During Postoperative Week 1, nausea, vomiting, sialorrhoea, and minor hematamesis occurred in 40, 25, 22, and 15 percent of patients, respectively. Symptoms disappeared spontaneously within 4 to 5 days and patients returned to normal activities 5 to 7 days postoperatively.
Mean total weight loss (TWL) at one, three, and six months postopertive was 11.2, 16, and 23 percent, respectively. The mean percentage of excess weight loss (EWL) at one, three, and six months postoperatively was 30.24, 43.9, and 48.58 percent, respectively.
Postoperative upper endoscopy and radiologic evaluation were only performed on four patients at one and four months due to reflux symptoms. Mild to moderate esophagitis was discovered and treated by long-term PPI and antacid.
Lumen size appeared stable at four months in patients who underwent upper endoscopy. In addition, two hiatal hernia (less than 4cm) were repaired; one case of cholecystectomy was performed; two gastric bands were removed and converted into placation; and one VBG was converted into plication.
Discussion/Conclusion
LGCP reduces the capacity of the stomach without cutting any part of it or using any device. Among all surgical procedures that reduce stomach capacity (i.e., SG, AGB, VBG) and which achieve around 50-percent EWL,[7] LGCP achieved this goal at six months in our series and others.[7,10,15–17]
All other current restrictive surgeries are accompanied by unsatisfactory weight loss that occurs in more than 20 percent of patients.[7,15,17] This failure rate requires surgery revision in up to 25 percent of patients.[7,15,17] In our series, surgery revision rate was 1.6 percent.
VSG is a primary bariatric procedure showing midterm results of 50- to 60-percent of EWL, with improvements in comorbidities. However, these results are associated with some complications, such as esophagitis, stenosis, fistulas, and gastric leaks near the angle of His. These leaks and fistulas are reported in nearly 2 to 5 percent of all operations.[16]
In our case series, gastric leak rate was 0.8 percent (one patient) and reoperation for complete obstruction rate was 0.8 percent (one patient).
Physiological concepts of LGCP are similar to VSG, which produces a smaller gastric pouch by folding the great curvature of the stomach, the fundus, the corpus, and the antrum. By folding and fixing the fundus, we have noticed less postoperative nausea and vomiting.
Clinical reports on LGCP demonstrate satisfactory EWL up to 65 percent.[15] In our series, we observed that early complications occurred less frequently than in other procedures (no cutting, no anastomosis, good calibration over a 32 French tube). It is early to compare results on EWL, but we can say that early complications are less frequent (0.8% leak rate) and less severe than other procedures.[18] All bleeding cases were managed intraoperatively and no postoperative bleeding occured. Our postoperative bleeding revision was nearly zero percent. This may be due to many factors (e.g., no gastric section, hemostasis control of trocar port was made at low peritoneal pressure after valsalva maneuver). In all cases, no drain was left in the operative site (hemostasis was performed by bipolar instrument).
Although the patent test made intraoperatively does not exclude the possibility of fold edema and complete obstruction of the residual gastric space, we continued performing this test to exclude mechanical obstruction after intragastric tube removal (elastic gastric effect suturing can cause complete collapse of residual lumen) and gastric distortion.
In our case series we found that fold edema was the most frequent complication (5%) specific to LGCP. It is easy to treat and regresses spontaneously within few days; however, it prolongs the patient’s hospitalization up to five days.
Leak after LGCP in our series was due to the following: 1) trauma due to the manipulation of the stomach when performing the LGCP and 2) early vomiting effort, which can cause rupture of stitches or herniation of the fold between stitches, thus leading to a leak by gastric distention.
Fixation of the fold occurs by suturing the gastric tissue between the point of entry of the needle at the posterior gastric wall and the point of exit of the needle at the anterior gastric wall in each point. This can reduce the incidence of leak and the fixation of the fundus can reduce the incidence of postoperative nausea and vomiting. Leaks after LGCP are much easier to manage than those occurring after VSG and RYGB[7,10] because LGCP is reversible, and there is enough gastric tissue to close the leak hole. Performing a new loose plication in case of peritonitis for the leak near the angle of His is feasible but challenging. Simple suturing of the gastric leak hole with the removal of the plication is another safe alternative.
Conclusion
Compared to other restrictive bariatric procedures, LGCP is a feasible, safe, and effective procedure for short-term EWL with low complication rates.
Safety, cost efficiency, and reversibility are the main decisive arguments in patient choice when choosing a restrictive procedure. Long-term results and more studies are needed to answer frequently asked questions by surgeons and patients about long-term results and weight regain after LGCP.
References
1. Gastrointestinal surgery for severe obesity: National Institutes of Health Consensus Development Conference Statement. Am J Clin Nutr. 1992;55(2 Suppl):615S–619S.
2. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004;292(14):1724–1737.
3. Nocca D, Frering V, Gallix B, et al. Migration of adjustable gastric banding from a cohort study of 4236 patients. Surg Endosc. 2005; 19(7):947–950.
4. Baltasar A, Bou R, Bengochea M, et al. Use of a Roux limb to correct esophagogastric junction fistulas after sleeve gastrectomy. Obes Surg. 2007; 17(10):1408–1410.
5. Martin LF, Smits GJ, Greenstein RJ. Treating morbid obesity with laparoscopic adjustable gastric banding. Am J Surg. 2007;194(3):333–343.
6. Gumbs AA, Gagner M, Dakin G, Pomp A. Sleeve gastrectomy for morbid obesity. Obes Surg. 2007;17(7):962–969.
7. Toouli J, Kow L, Ramos AC, et al. International multicenter study of safety and effectiveness of Swedish adjustable gastric band in 1-, 3-, and 5-year follow-up cohorts. Surg Obes Relat Dis. 2009;5:598–609.
8. Fusco PE, Poggetti RS, Younes RN, et al. Evaluation of gastric greater curvature invagination for weight loss in rats. Obes Surg. 2006;16(2):172–177.
9. Fusco PE, Poggetti RS, Younes RN, et al. Comparison of anterior gastric wall and greater gastric curvature invaginations for weight loss in rats. Obes Surg. 2007;17(10):1340–1345.
10. Talebpour M, Amoli BS. Laparoscopic total gastric vertical plication in morbid obesity. J Laparoendosc Adv Surg Tech A. 2007;17(6):793–798.
11. Sales Puccini, CE. Sales’ gastric surset: a new alternative in bariatric restrictive surgery. Rev Colomb Cir. 2008;23(3):131–135.
12. Brethauer SA, Harris JL, Chand B, et al. Initial results of vertical gastric plication for severe obesity. Presented at: Society of American Gastrointestinal and Endoscopic Surgeons. Phoenix, Arizona. April 22–25, 2009.
13. Galvao M, Ramos AC, Campos JM, et al. Endoscopic removal of eroded adjustable gastric band. Lessons learned after 5 years and 78 cases. Surg Obes Relat Dis. 2011. In Press
14. Campos JM, Siqueira LT, Meira MR, et al. Gastrobronchial fistula as a rare complication of gastroplasty for obesity: a report of two cases. J Bras Pneumol. 2007;33(4):475–479.
15. Ramos A, Galvão M, Campos JM, Mottin CC. Laparoscopic greater curvature plication: an Alternative restrictive bariatric procedure. Bariatric Times. 2010;7(5):8–10.
16. Clinical Issues Committee of the American Society for Metabolic and Bariatric Surgery, Updated Position Statement on Sleeve Gastrectomy as a Bariatric Procedure. Surg Obes Relat Dis. 2010;6(1):1–5. Epub 2009 Nov 17.
17. Brethauer SA, Harris JL, Kroh M, Schauer PR. Laparoscopic gastric plication for treatment of severe obesity. Surg Obes Relat Dis. 2011;7(1):15–22. Epub 2010 Nov 9.
18. Campos GM, Rabl C, Roll GR, et al. Better weight loss, resolution of diabetes, and quality of life for laparoscopic gastric bypass vs banding: results of a 2-cohort pair-matched study. Arch Surg. 2011;146(2):149–155.
Category: Case Series, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}