
Endoluminal Management of Morbid Obesity
by Matthew J. Kruse, MD, and Miguel A. Burch, MD, FACS
Dr. Kruse is from the Division of General Surgery, Department of Surgery, Cedars-Sinai Medical Center, Los Angeles, California. Dr. Burch is Associate Director of General Surgery and Minimally Invasive Surgery, Department of Surgery, Cedars-Sinai Medical Center, Los Angeles, California
Funding: There was no funding for the development of this article.
Financial Disclosures: The authors reports no conflicts of interest relevant to the content of this article.
Bariatric Times. 2010;7(9):8–12
Abstract
Objective. The significant health consequences and ever-growing prevalence of obesity in developed countries, combined with convincingly positive results of bariatric surgery, has led to amplified interest in less invasive and more accessible interventional treatment strategies. Several available endoscopic procedures are both designed after and intended to reproduce the results of various bariatric surgical procedures. This article summarizes the rationale, execution, efficacy, and complications of commonly performed endoluminal bariatric procedures, based on currently available evidence. A brief overview of alternative techniques still in development is also included. Design. A literature review of current techniques and available outcome data was conducted, with supplemental comment from the authors’ personal experience. Results. Commonly employed endoluminal bariatric procedures include placement of space-occupying intragastric balloons, gastroplasty techniques using endoscopic suturing or stapling devices, and deployment of malabsorptive bypass sleeves in the proximal small intestine. Methods. Preliminary stages of research include implantable gastric stimulators and intragastric botulinum toxin injection. Conclusions. The expanding field of endoluminal bariatric procedures shows promise in effective short-term weight loss with rare major complications. Long-term data are sparse, however, and further studies are needed to evaluate and define the proper role for endoscopic procedures in the treatment of obesity.
Introduction
The realization of the minimally invasive revolution and its impact on patient outcomes, especially in the bariatric population, has spurred interest in developing less invasive options for surgical therapy. This interest led to several ventures into experimental endoscopic procedures that transgress the gastrointestinal lumen into the peritoneum to, in effect, perform laparoscopic surgery or so-called natural orifice transluminal endoscopic surgery (NOTES). Although significant progress has been made by select centers, the generalizability of these techniques awaits significant evolution of the basic endoscope as well as its effector instruments. Additionally, transgression of the gastrointestinal (GI) lumen creates an inherent risk of leakage, as there is a perforation to close at the conclusion of these procedures. The target organs in weight loss surgery are within easy reach of standard endoscopes and as such are amendable to endoluminal endoscopic manipulation without breaching the GI lumen. To this end, several platforms are available or in the late phase clinical trials for endoscopic bariatric surgery.
To date, no medical therapies exist that match the impact demonstrated by bariatric surgery on reduction in weight, comorbidity control or mortality reduction.[1] These results, along with continuously improving techniques and training of bariatric surgeons, have increased the access to weight loss surgery.[2] It has been shown that preoperative weight reduction is an important adjunct to better perioperative outcomes.[3] However, achieving significant preoperative weight loss can prove challenging for certain subgroups of patients. Still, other patient populations are not interested in laparoscopic bariatric surgery but need to lose weight for comorbidity control prior to other surgical interventions, such as joint replacement or abdominal wall reconstructions. These patients would benefit from procedure-based weight loss as a bridge to their eventual procedures.
This article will describe the currently available endoscopically based platforms for weight loss and summarize data from clinical trials and early clinical series published in the literature. The current selection of endoluminal weight loss procedures can be classified as restrictive or malabsorptive, based upon the main mechanism of action.
RESTRICTIVE
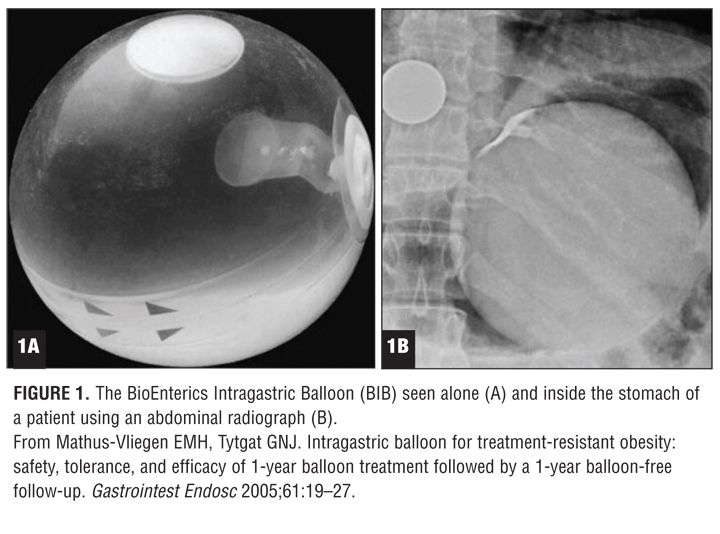
Balloon-based techniques. The earliest form of endoluminal bariatrics was the placement of space-occupying gastric balloons. In 1982, Nieben and Harboe[4] reported the placement of a thin-walled balloon into the stomachs of five women with obesity. They noted an average weight loss of 5kg during periods that the balloons remained inflated. When the balloons eventually ruptured spontaneously, they would pass in the stool and another balloon would be placed.[4] The outcomes of these first generations of gastric balloons were disappointing with poor weight loss and significant complications including balloon migration with resultant obstructions, gastric ulceration, and perforation.[5,6] Significant design evolution has resulted in acid-resistant balloons that are saline filled to higher capacities, are no longer cylindrical, and now come in various spherical shapes. Modern balloon insertion techniques vary. In general, the collapsed balloons, stiffened by a guide wire, are advanced into the stomach much as a nasogastric tube. Once in the stomach they are endoscopically evaluated and inflated to varying volumes (ranging from 400–800cc) depending on the manufacturer. Removal is performed by endoscopic deflation of the devices either by needle deflation through a repenetrable valve or needle puncture and removal with baskets or a snare.
Although there are several balloons in various stages of trials and clinical use, the Bioenterics Intragastric Balloon (BIB®—Allergan, Irvine, California) has been the most studied (Figure 1). The largest report included 2,515 patients who had the BIB placed between 2000 and 2004.[7] They were predominately women with a mean body mass index (BMI) of 44.8±07.8 who were followed for a period of six months. Outcomes demonstrated promising results: the six-month percentage of excess weight loss (EWL) was 33.9±18.7, and improvement or resolution of hypertension and diabetes was observed in 86.9 and 93.7 percent, respectively. Complications on insertion were reported rarely (0.08%), and were related to acute gastric dilatation. Removal of the balloon was necessary in 11 (0.44%) patients within the first month for psychological intolerance—a term not clearly characterized in the original manuscript. The overall complication rate was quoted as 2.8 percent (70 out of 2,515) but the nature of these complications were not all described. There were five patients who experienced perforations related to the balloon, four of whom had previous gastric surgery. Two of these four patients died. Of the six patients who had previously undergone gastric surgery, four experienced perforations, and two of those died, implying that previous gastric surgery could be a contraindication to balloon placement.
A double-blind, randomized, controlled, crossover study revealed the likely efficacy of the device by using patients as their own blinded controls.[8] In this study, 32 patients were randomized into a BIB group or a sham group. Their weight loss was tracked for three months and then the patients underwent repeat endoscopy where the BIB patients had their balloons removed and those who had previous been sham patients had a BIB placed. Their weights were watched and a final endoscopy was performed again for three months. Group A (BIB to sham) had a mean of 34.0±4.8 percent EWL at three months and 4.6±1.1 percent EWL during the Sham portion of their trial. Group B (sham to BIB) had a mean of 2.1±1.0 percent EWL during the sham and 31±4.8 percent EWL once crossed over to the BIB portion of their trial.
To date, there are no intragastric balloons approved for use in the United States, although a search of clinicaltrials.gov revealed at least two United States trials underway, which include the following: “A Study of BioEnterics® Intragastric Balloon (BIB®) System to Assist in the Weight Management of Obese Subjects (NCT00730327)” and “The Safety and Efficacy of the ReShape Intragastric Balloon in Obese Subjects (NCT01061385).” Although there appears to be a benefit to the balloons for weight loss, studies seem to indicate that the long-term weight loss is dependent on the balloon presence, thus its long term utility is still unknown. It would appear a potential candidate for bridging therapy, as a function of enhanced weight loss and comorbidity reduction.
Gastroplasty-based techniques. Vertical banded gastroplasty is historically an important bariatric procedure that provided significant and durable weight loss in some patients. The procedure created a narrow tube along the lesser curvature beginning at the cardia and ending with a band at the end of this tube to aid in the sense of restriction and satiety. The continued development of endoscopic platforms for tissue molding and apposition led to the first endoscopic stapling device, which was capable of creating full-thickness plications. The Transoral Gastroplasty device [(TOGA) (Satiety, Inc. Palo Alto, California)] is capable of producing a long, thin gastric sleeve based off the lesser curvature with additional plications at the end of this sleeve for additional restriction—a procedure similar in design to the vertical gastroplasty. The procedure begins with the endoscopic placement of a guide wire over which the 54 French device, termed a sleeve stapler, is introduced into the proximal stomach. Once its position is confirmed endoscopically, a “sail-septum” is deployed to stabilize the anterior and posterior walls of the body and greater curvature and prevent their incorporation into the sleeve. Suction pods located within the stapling device are activated bringing lesser curvature tissue within the jaws of the device. The stapler is then fired, creating the narrow sleeve, and the maneuvers are repeated to create an 8–9cm long sleeve. At the end of this sleeve, a smaller stapling device is used to create additional resistance to flow. Initial trials revealed a variable weight loss from 24.4 to 46.0 percent EWL at six months. Endoscopies at the end of the trial period revealed partial dehiscence of the staple lines. Improvements led to the second-generation device demonstrating an intact staple line in 7 of 11 patients at six months, compared with only 5 of 21 patients treated with the first-generation device.[9,10] The decreased rate of staple-line dehiscence in the second generation device likely contributed to a more stable EWL of 46.0 percent at six months in the latest published trial.[9] No major adverse events were reported in the early trials. Insulin sensitivity has been shown to increase as soon as three months after the procedure.[11]
The use of this technology as a bridge to further weight loss surgery appears less clear, as the placement of full-thickness staple lines raises questions of subsequent management of failures from TOGA. Closset et al12 reported conversion from TOGA to laparoscopic gastric bypass in four patients.[12] All were for inadequate weight loss, two with endoscopically intact TOGA staple lines, two with dehiscence in the line. During laparoscopy they reported no evidence of a visible serosal staple line in the patients with dehiscense and a visible invagination in those with intact TOGA staple lines. Additionally, they reported no evidence of adhesions to the invaginations. The gastric bypasses were conducted using a 32 French bougie to size the pouch. When visible, the TOGA staple lines were excluded from the pouch. They reported no significant increases in operating time (ascribed to no adhesions) and no postoperative leaks.
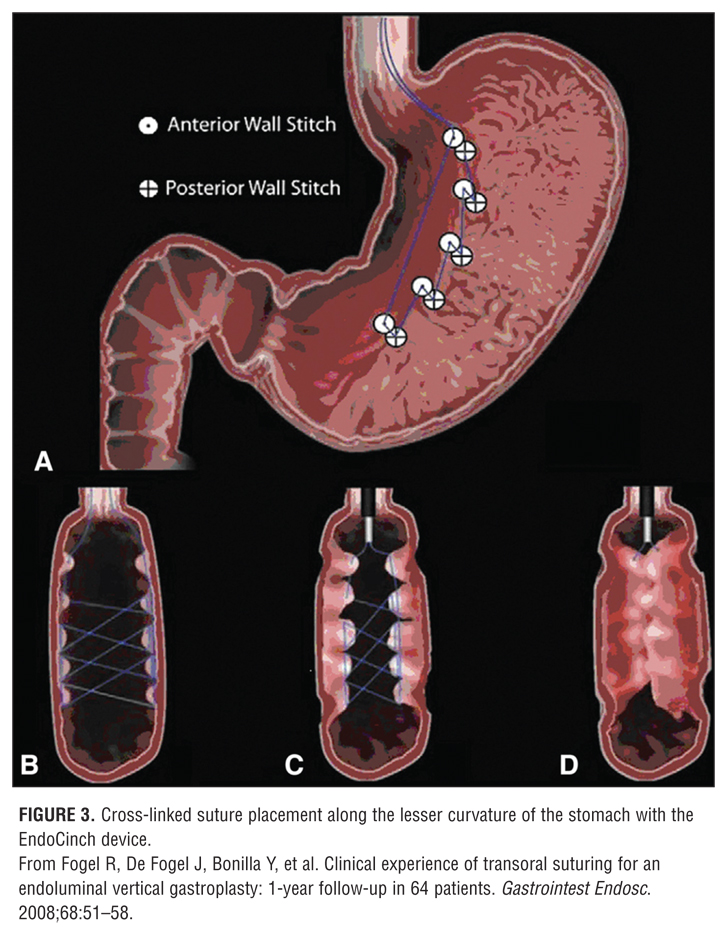
Another option for gastric plication is the EndoCinch device (C.R. Bard, Murray Hill, New Jersey). Originally developed as an endoscopic treatment for gastroesophageal reflux, the overtube-based device used a suction chamber to capture the stomach wall. The tissue in the chamber then had a suture passed through it allowing for rudimentary suturing of the gastric wall. When used for gastroesophageal reflux disease (GERD), pleats were created at the gastroesophageal junction in an effort to prevent the reflux of fluid from the stomach. However, long-term durability of the procedure was questionable, owing to the fact that the sutures did not appear to be full thickness, and thus, with time, the pleats were lost.[13] Fogel et al[14] used the first generation of the device to place several sutures to plicate the greater curvature, thus decreasing the distensibilty and overall volume of the stomach (Figure 4). Short-term results demonstrated effective weight loss in 64 patients who had the procedure, with 21.1 percent EWL at one month and 58.1 percent EWL at 12 months. Only 14 patients received endoscopy in follow up, and 11 of 14 had intact plication sutures. A newer generation of this same device, RESTORe Suturing System™, is currently under investigation in a clinical trial [Transoral Gastric Volume Reduction as an Intervention for Weight Management (TRIM) NCT00679848] for gastric volume reduction.
MALABSORPTIVE
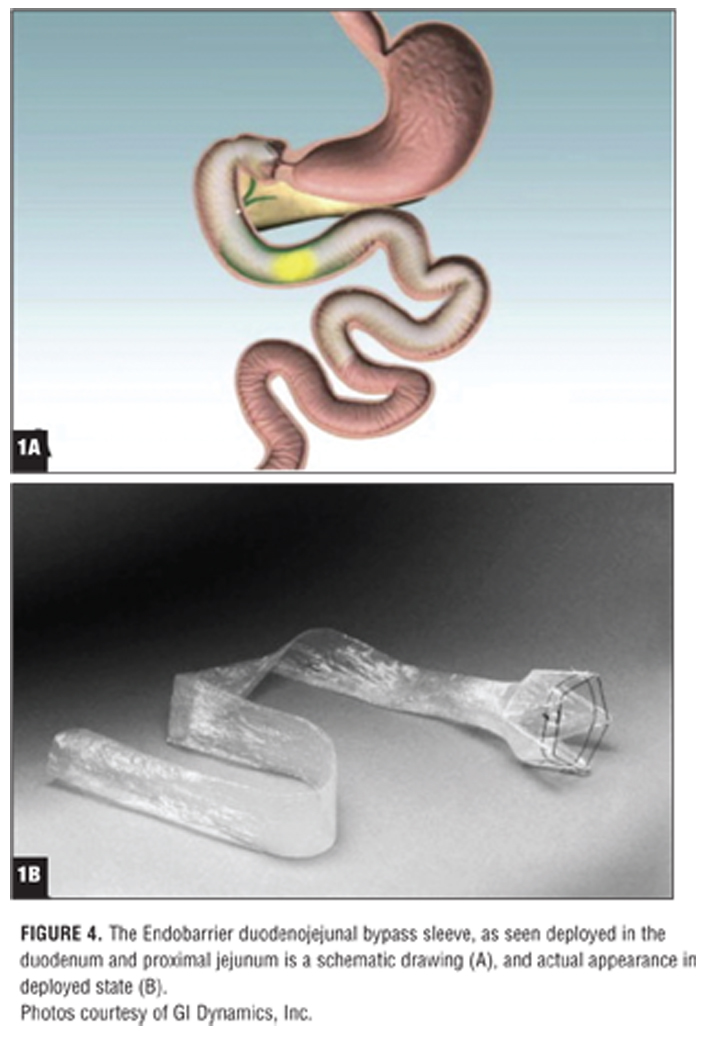
Duodenal-jejunal bypass sleeve/liner. The dramatic hormonal alterations seen with bypassing of the duodenum and proximal jejunum are challenging our understanding of the mechanisms underlying gastric bypass surgery. In particular, the improvement in insulin sensitivity and glucose metabolism seen with gastric bypass can occur immediately after surgery, well before any significant weight loss has occurred. Implantation of the duodenojejunal bypass sleeve (DJBS), now called “the Endobarrier” (GI Dynamics, Inc., Watertown, Massachusetts) is designed as a means of malabsorptive weight loss by bypassing the duodenum and proximal jejunum through deployment of a plastic sleeve. The sleeve itself is a 60cm, impermeable, fluoropolymer liner anchored in the proximal duodenum by a self-expanding nitanol fastener (Figure 4). Once in place, food passes through the sleeve without mixing with biliopancreatic juices or touching the brush border of the jejunum.
The initial human study demonstrated 23.6 percent EWL at three months, with immediate improvement in blood glucose concentration in 3 of 4 patients with baseline type 2 diabetes mellitus (T2DM).[15] In a subsequent small, randomized, controlled trial assigning patients to either a low-fat diet or the DJBS device, the researchers found that at three months EWL was 22 percent for the device group compared to 5.0 percent for the control group.16 In both trials, patients with T2DM had better glucose metabolism, promising perhaps a new adjunct to diabetes management in patients with morbid obesity. A more recent controlled trial studying shams showed an EWL of 11.9 percent in the 21 patients randomized to the treatment arm versus 2.7 percent in the sham group.[17]
Although demonstrating promising weight loss results, all trials have had to contend with early discontinuation of device use. In the sham-controlled trial, eight subjects terminated early because of gastrointestinal bleeding (n=3) or device intolerance (pain and/or vomiting; n=4) and an unrelated preexisting illness (n=1). Of the three patients with GI hemorrhage, 2 out of 3 patients required blood transfusions. Similarly, in other earlier trials, patients required early device retrieval for upper GI bleed, migration, or sleeve obstruction.[16,18] Despite its challenges, the device offers an innovative potential bridge to patients preparing for surgery and who require tighter diabetes control as well as weight loss.
Technology on the Horizon
A number of other devices are in varying stages of development for use as endoluminal platforms. The ValentX bypass sleeve (ValenTx, Inc., Carpinteria, California) is another endoscopically placed removable sleeve designed for malabsorptive weight loss. It is placed not in the duodenum but at the gastroesophageal junction, thus bypassing the stomach as well. An initial trial of 12 patients presented at the 2009 American College of Surgeons Clinical Congress demonstrated 39.5 percent EWL at 12 weeks.[23]
Alternative endoscopic bariatric interventions include implantable electrical gastric stimulators and intragastric administration of botulinum toxin. Implantable gastric stimulators have been associated with weight loss[19] and endoscopic implantation of temporary stimulators has been shown feasible.[20] Endoscopically placed, gastric stimulators are under development for the purpose of treating obesity. However, a recent randomized, controlled trial of gastric stimulation showed no difference in weight loss at 12 months compared to diet and behavioral therapy.[21]
Endoscopic intragastric injection of botulinum toxin has been studied as a method of weight loss in patients with obesity, working by the proposed mechanism of increased gastric emptying time and reduced food intake. A randomized, controlled trial of 24 patients concluded that endoscopic injection of botulinum toxin resulted in significantly increased weight loss compared to placebo (11±1.09kg vs. 5.7±1.1kg) after eight weeks, as well as significantly greater prolongation in gastric emptying time (+18.93±8 vs -2.2±6.9 min, P<0.05).[22] Further studies would be needed to evaluate the efficacy, safety, and long-term effects of these modalities in larger patient populations.
In summary, several potential endoscopically delivered platforms exist that effect weight loss at a level above that seen with standard dieting. The expanding field of endoluminal bariatric procedures shows promise in effective short-term weight loss, with rare major complications. Long-term data are sparse, however, and further studies are needed to evaluate and define the proper role for endoscopic procedures in the treatment of obesity.
Figure 1
Figure 2
Figure 3
Figure 4
References
1. Sjöström L, Narbro K, Sjöström CD, et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007;357(8)741–752.
2. DeMaria EJ, Pate V, Warthen M, Winegar DA. Baseline data from American Society for Metabolic and Bariatric Surgery—designated bariatric surgery centers of excellence using the Bariatric Outcomes Longitudinal Database. Surg Obes Relat Dis. 2010;6(4):347–355.
3. Benotti PN, Still CD, Wood GC, et al. Preoperative weight loss before bariatric surgery. Arch Surg. 2009;144(12):1150–1155.
4. Nieben OG, Harboe H. Intragastric balloon as an artificial bezoar for treatment of obesity. Lancet. 1982;1(8265):198–199.
5. Lindor KD, Hughes RW Jr, Ilstrup DM, Jensen MD. Intragastric balloons in comparison with standard therapy for obesity—a randomized, double-blinded trial. Mayo Clin Proc. 1987;62(11):992–996.
6. Benjamin SB, Maher KA, Cattau EL Jr, et al. Double-blind controlled trial of the Garren-Edwards gastric bubble: an adjunctive treatment for exogenous obesity. Gastroenterology. 1988;95(3):581–588.
7. Genco A, Bruni T, Doldi SB, et al. BioEnterics Intragastric Balloon: the Italian experience with 2,515 patients. Obes Surg. 2005;15:1161–1164.
8. Genco A, Cipriano M, Bacci V, et al. BioEnterics Intragastric Balloon (BIB): a short-term, double-blind, randomised, controlled, crossover study on weight reduction in morbidly obese patients. Int J Obes. 2006;30(1)129–133.
9. Moreno C, Closset J, Dugardeyn S, et al. Transoral gastroplasty is safe, feasible, and induces significant weight loss in morbidly obese patients: results of the second human pilot study. Endoscopy. 2008;40:406–413.
10. Deviere J, Ojeda Valdes G, Cuevas Herrera L, et al. Safety, feasibility and weight loss after transoral gastroplasty: first human multicenter study. Surg Endosc. 2008;22:589–598.
11. Chiellini C, Iaconelli A, Familiari P, et al. Study of the effects of transoral gastroplasty on insulin sensitivity and secretion in obese subjects. Nutr Metab Cardiovasc Dis. 2010;20(3):202–207.
12. Closset J, Germanova D, Loi P, et al. Laparoscopic gastric bypass as a revision procedure after transoral gastroplasty. Obes Surg. 2009 Dec 10. [Epub ahead of print].
13. Schiefke I, Zabel-Langhennig A, Neumann S, et al. Long-term failure of endoscopic gastroplication (EndoCinch). Gut. 2005;54:752–758.
14. Fogel R, De Fogel J, Bonilla Y, et al. Clinical experience of transoral suturing for an endoluminal vertical gastroplasty: 1-year follow-up in 64 patients. Gastrointest Endosc. 2008;68:51–58.
15. Rodriguez-Grunert L, Galvao Neto MP, Alamo M, et al. First human experience with endoscopically delivered and retrieved duodenal-jejunal bypass sleeve. Surg Obes. Relat Dis 2008;4:55–459.
16. Tarnoff M, Rodriguez L, Escalona A, et al. Open label, prospective, randomized controlled trial of an endoscopic duodenal-jejunal bypass sleeve versus low calorie diet for pre-operative weight loss in bariatric surgery. Surg Endosc. 2009;23:650–656.
17. Gersin KS, Rothstein RI, Rosenthal RJ, et al. Open-label, sham-controlled trial of an endoscopic duodenojejunal bypass liner for preoperative weight loss in bariatric surgery candidates. Gastrointest Endosc. 2010;71:976–982.
18. Schouten R, Rijs CS, Bouvy ND, et al. A multicenter, randomized efficacy study of the EndoBarrier Gastrointestinal Liner for presurgical weight loss prior to bariatric surgery. Ann Surg. 2010;251(2):236-43.
19. Cigaina V. Long-term follow-up of gastric stimulation for obesity: the Mestre 8-year experience. Obes Surg. 2004;14 (Suppl 1):S14–22.
20. Liu J, Hou X, Song G, et al. Gastric electrical stimulation using endoscopically placed mucosal electrodes reduces food intake in humans. Am J Gastrenterol. 2006;101(4);798–803.
21. Shikora SA, Bergenstal R, Bessler M, et al. Implantable gastric stimulation for the treatment of clinically severe obesity: results of the SHAPE trial. Surg Obes Relat Dis. 2009;5(1)31–37.
22. Foschi D, Corsi F, Lazzaroni M, et al. Treatment of morbid obesity by intraparietogastric administration of botulinum toxin: a randomized, double-blind, controlled study. Int J Obes. 2007;31(4):707–712.
23. Sandler B, Horgan S, Jacobsen G. Human experience with endoluminal endoscopic gastro-duodeno-jejunal bypass sleeve. Presented at the 95th Annual American College of Surgeons Clinical Congress. Chicago, IL. October 13th, 2009.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
This topic will be discussed at the upcoming 4th Annual UCSD Hands-On NOTES & Single Site Surgery Symposium. Please register for the symposium if you are interested in receiving more information on this important topic.