
How to Perform a Roux-en-Y Gastric Bypass Using the Circular Stapler
Surgical Pearls: Techniques in Bariatric Surgery
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS and Daniel B. Jones, MD, MS, FACS
This month’s technique: How to Perform a Roux-en-Y Gastric Bypass Using the Circular Stapler
This Month’s Featured Expert: Alan C. Wittgrove, MD, FASMBS
Dr. Wittgrove is Medical Director, Wittgrove Bariatric Center, La Jolla, California
Bariatric Times. 2011;8(8):8–9
At University of California San Diego (UCSD) and Scripps Memorial Hospital, La Jolla, California, I perform Roux-en-Y gastric bypass (RYGB) using the circular stapler. Here, I will describe the procedure step-by-step using one patient case as an example for preparation.
Preparation
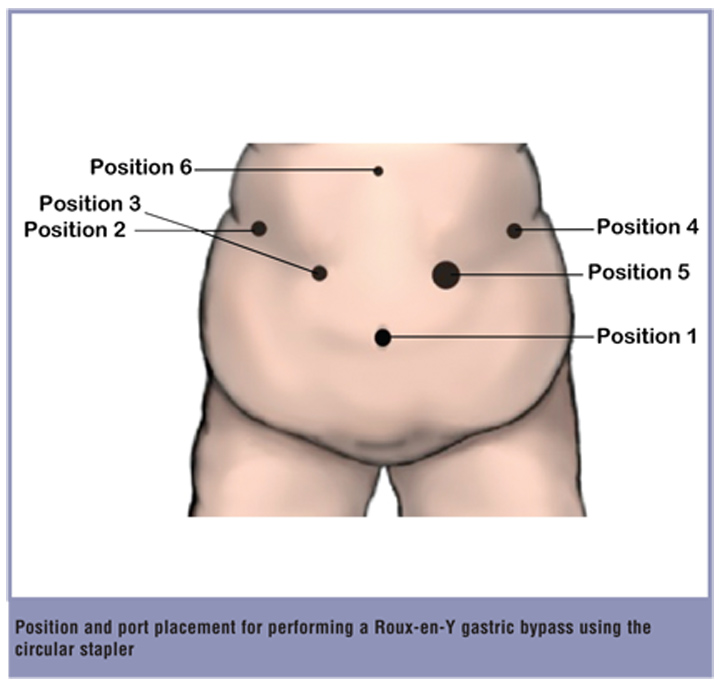
To begin the procedure, the patient was laid in a supine position. Pneumoperitoneum to 17mmHg was established by a Veress needle in the left upper quadrant just below the subcostal line. The first 12mm trocar (position 1) was placed in the midline at the umbilicus. Four 12mm trocars were placed in the standard positions for this particular operation: in the right upper quadrant subcostal area along the mid-clavicular line (position 2), a handbreadth inferior to the second port along the line joining this port to the umbilicus (position 3), in the left upper quadrant subcostal area along the midclavicular line (position 4), and one handbreadth inferior and vertically below the fourth port (position 5). It is important to note that for this procedure, position 5 is changed to a 21mm opening to fit the Stealth 21mm stapling device (Ethicon Endo-Surgery, Cincinnati, Ohio). A 5mm trocar was also placed in the subxiphoid area for the placement of the liver retractor (position 6). We routinely use a ratcheted grasper with teeth and secure it to the left crus to elevate the left lobe of the liver and appropriately visualize the hiatus.
Procedure
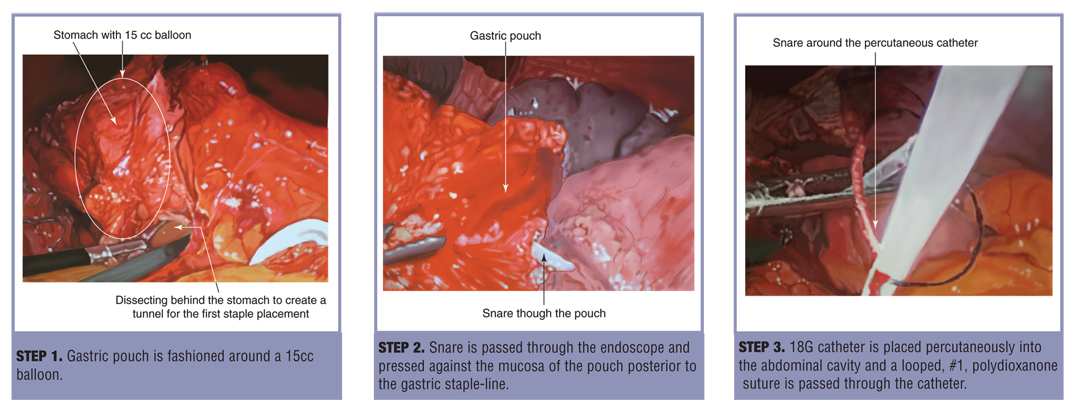
Steps 1 through 3
The first step of performing the RYGB using a circular stapler is entry into the lesser sac through the gastrohepatic ligament with placement of a penrose drain. Next, the transverse mesocolon is elevated and the penrose drain is brought into the inframesocolic compartment through an incision at the base of the mesentery. This will be the point through which the Roux limb will be brought into the supramesocolic compartment. The ligament of Treitz is identified and the jejunum is divided 10cm distally using a linear cutting stapler with a Blue load. A 75cm Roux limb is measured. A side-to side anastomosis is created using a white load stapler. The small bowel mesenteric space is closed using nonabsorbable suture (Pare Systems). The penrose drain is sutured to the Roux limb and the intestine is brought through the lesser sac into the upper abdomen.
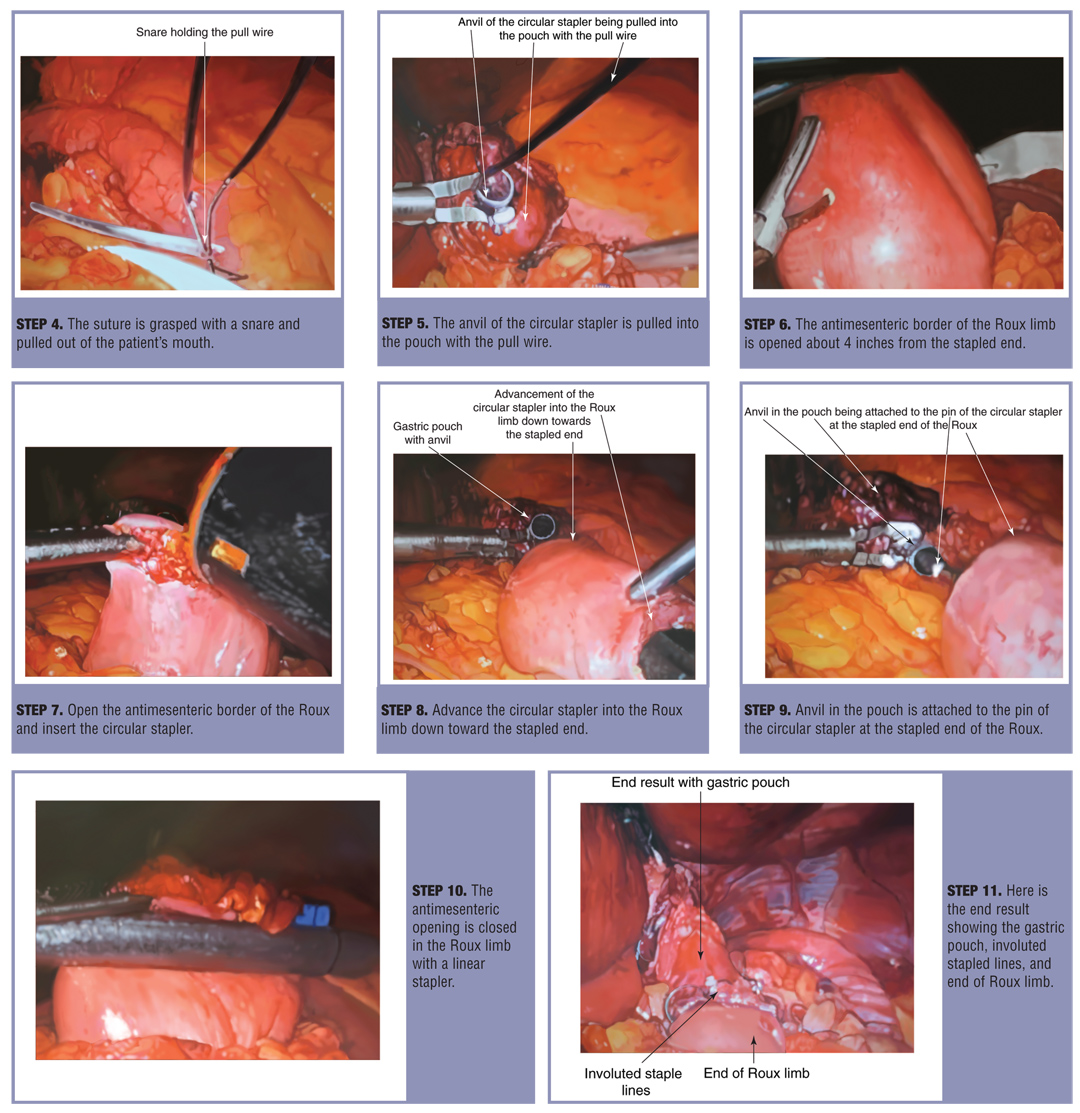
The hiatus is dissected out carefully using electrocautery or harmonic as appropriate. The angle of His is exposed. Any hiatal hernia is repaired in a posterior fashion. The gastric pouch is fashioned around a 15cc balloon passed by the anesthesiologist. An upper endoscopy is performed using a standard 10mm video endoscope. A snare is passed through the endoscope and pressed against the mucosa of the pouch posterior to the gastric staple line. Electrocautery is used to open onto the snare, allowing it to be seen within the abdominal cavity with the laparoscope. An 18G catheter is then placed percutaneously into the abdominal cavity and a looped, #1, polydioxanone (PDS) suture is passed through the catheter. This suture is grasped with a snare and pulled out of the patient’s mouth. The anvil of a Stealth 21mm stapling device (Ethicon Endo-Surgery) is attached to the looped PDS and the anvil is pulled down into the small gastric pouch. Endoscopic evaluation has shown no evidence of damage to the esophagus with this technique. A small counter-incision is then carried out on the anti-mesenteric border of the small intestine, several inches from the stapled end of the Roux limb. The circular stapler is introduced through the abdominal wall on the patient’s left side and introduced into the bowel lumen through the antimesenteric opening. The stapler is advanced to the stapled end of the Roux limb, connected to the anvil and the gastrojejunal (GJ) anastomosis is created in an end-to-end fashion. The opening for the introduction of the Stealth stapler is closed with a linear 45mm stapling device. Three sutures are placed anteriorly to involute any potential ischemic tissue between the gastric staple line and the stable line of the GJ anastomosis. The proximal Roux limb is cross-clamped with an atraumatic bowel clamp and a final endoscopy is performed to rule out leak.
Discussion
Using this technique we have had a stricture rate of between 3 and 5 percent. Since the GJ anastomosis is end to end, dilation is less complicated. There is no affarent or “blind limb” of small bowel for the dilating catheter to mistakenly go down. The pouch is very small so pouch enlargement over time is minimal.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}