
How to Perform an Evaluation and Reduction of Internal Hernia Via a Laparoscopic Single Incision
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS, and Daniel B. Jones, MD, MS, FACS
This column recruits expert surgeons to share step-by-step technical pearls on bariatric procedures.
This Month’s Technique: How to Perform an Evaluation and Reduction of Internal Hernia Via a Laparoscopic Single Incision
This Month’s Featured Expert: Michael A. Schweitzer, MD, Department of Surgery, The Johns Hopkins University School of Medicine, Baltimore, Maryland
Bariatric Times. 2011;8(12):8–9
Co-Authors: Katherine Graw Lamond, MD, Minimally Invasive Surgery Fellow, The Johns Hopkins University School of Medicine, Baltimore, Maryland; and Kimberley E. Steele, MD, FACS, Assistant Professor of Surgery, The Johns Hopkins University School of Medicine, Baltimore, Maryland
Funding: There was no funding for the preparation of this manuscript.
Disclosures: The authors reports no conflicts of interest relevant to the content of this manuscript.
Introduction
At Johns Hopkins Bayview Medical Center in Baltimore, Maryland, we typically perform laparoscopic antecolic antegastric Roux-en-Y gastric bypass (RYGB). The antecolic approach creates two mesenteric defects: jejunojenostomy, also called entero-enterostomy, and “Petersen’s” defects, which are both closed during the index operation with nonabsorbable sutures (Surgidac, Covidien, North Haven, Connecticut). The retrocolic RYGB approach creates the two aforementioned defects as well as a third mesenteric defect through the transverse mesocolon. I provide a step-by-step method of diagnosing and repairing an internal hernia using a minimally invasive approach.
Evaluation
Patients with internal hernias typically present with recurrent intermittent peri-umbilical abdominal pain, that may be described as “cramping” in nature. Abdominal computerized axial tomography (CAT) scan may reveal a “swirling” mesentery, small bowel obstruction, or completely be unremarkable. Therefore, it may be necessary to do a diagnostic laparoscopy if internal hernia is suspected despite a normal CAT scan.
Preparation
The patient should be placed on the operative table in the supine position. A supraumbilical curvilinear 3cm incision is performed (see Figure 1). Fascia is opened under direct vision approximately 3cm in order to facilitate entry with a single-site port, such as a SILS port (Covidien). The abdomen is inflated to 15mmHg and a 5mm 45-degree long laparoscope along with two 5mm bowel graspers are also inserted through the single port (see Figure 1.)
Procedure
Evaluation of gastric pouch and Roux limb. After instrumentation has been placed into the abdomen, the first step is to identify the Roux limb. Unless there is suspicion of problems with the gastrojejunostomy or gastric pouch on preoperative studies, it may not be necessary to investigate this area if the amount of adhesions that need to be lysed does not warrant the risk of injury. While it is common over time for the Roux limb to dilate, it is still important to rule out any kinks, strictures, or adhesive bands that may be causing an obstruction, especially near the entero-enterostomy.
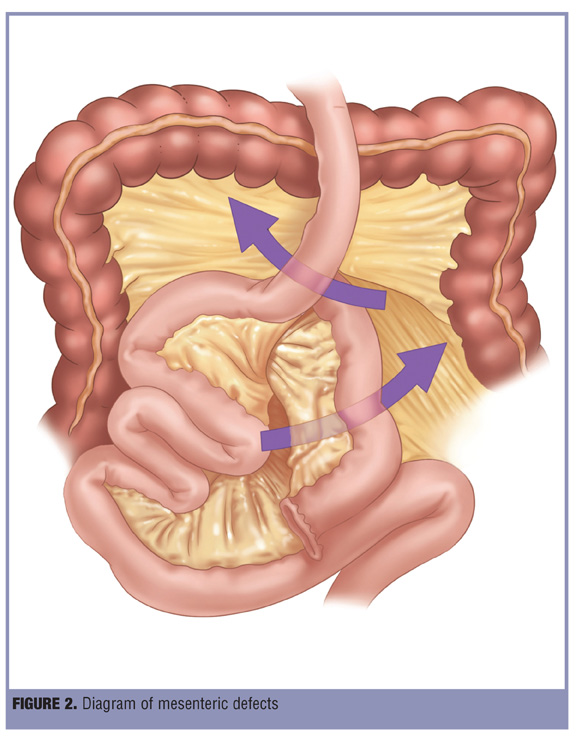
Evaluation of “Petersen’s” space. The “Petersen’s” space is the region created between the transverse mesocolon and the Roux limb mesentery (see Figure 2).
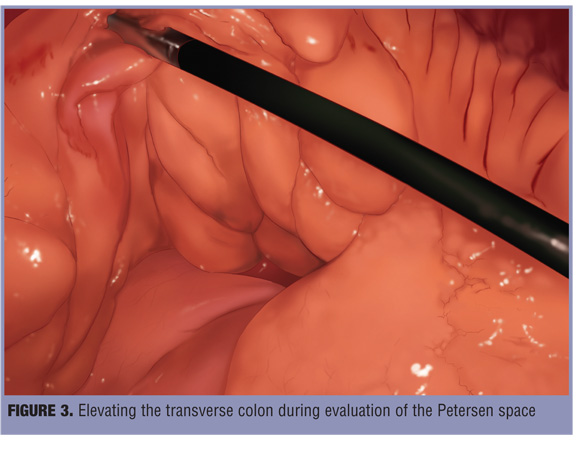
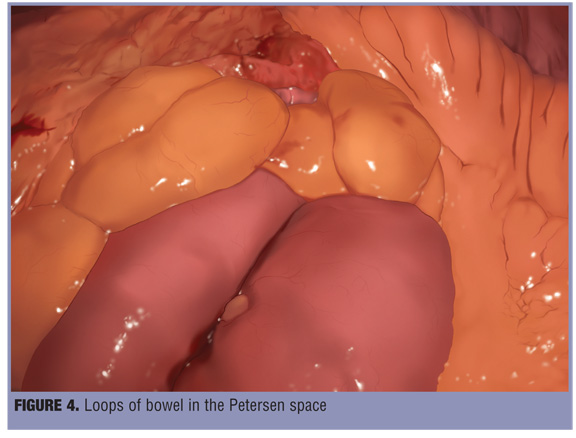
Typically, this space is closed with a running suture in order to deter any loops of small bowel from entering the space and becoming twisted or stuck. This space can be best evaluated by elevating the transverse colon (see Figure 3) as well as the Roux limb. If there are loops of bowel in this space (see Figure 4), they can be reduced by gently grasping the bowel loops. The defect can then be closed with interrupted or running sutures.
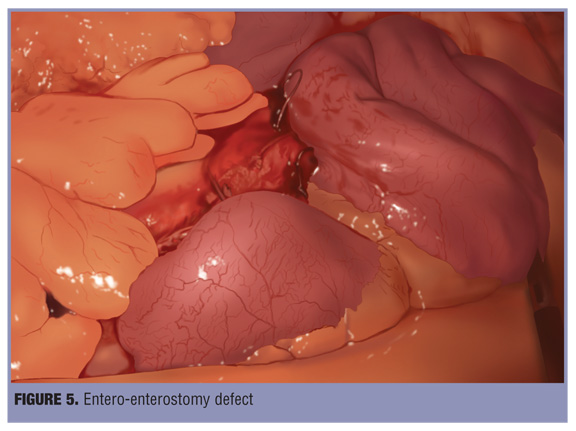
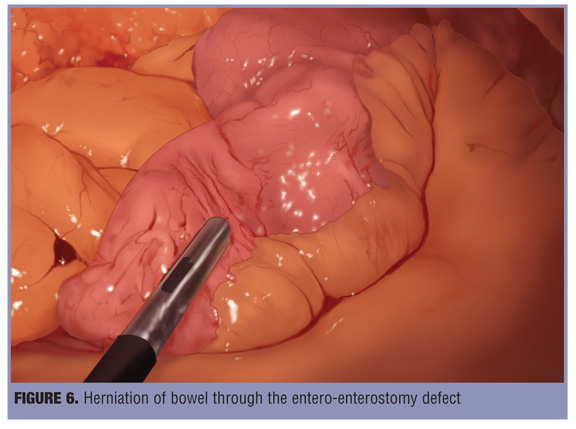
Evaluation of the entero-enterostomy defect. The Roux limb is followed distally in order to visualize the entero-enterostomy defect (see Figure 2 and Figure 5). At times, bowel can be herniated through the mesenteric defects and adhesions can form (see Figure 6). It is important to carefully release these adhesions so that the small bowel can be completely reduced. If adhesions make it difficult to find the jejunal anastomosis or the incarcerated bowel is difficult to reduce, then it may be easier to locate the ileocecal junction and trace the common channel small bowel proximally to the anastomosis. In most cases, the incarcerated small bowel will reduce by gently pulling the common channel away from the entero-enterostomy.
The defect can best be evaluated by carefully elevating the entero-enterostomy, allowing better visualization of the mesentery. Even if there is no herniated bowel discovered in this space, it is important to close the defect so that the small bowel cannot intermittently herniate through and cause symptoms.
Once the defects are closed, the biliopancreatic limb can be followed back to the ligament of Treitz to ensure that there are no kinks or strictures.
Evaluation of the transverse mesocolon defect. At this time, if the patient has a retrocolic Roux limb, it is important to evaluate the transverse mesocolon defect.
It is important not to close this defect too tightly, so that there is not an obstruction created at the Roux limb.
Conclusion
Mesenteric defects can be a source of potentially serious complications in laparoscopic gastric bypass patients. Single-incision surgery can be utilized to assist in operative evaluation. The key steps include running the small bowel and intracorporeal suturing, which can all be accomplished through a single incision with multiple ports (Figure 1,Figure 2, Figure 3, Figure 4, Figure 5, Figure 6, Figure 7). If difficulty is encountered, other laparoscopic ports can be placed or the procedure can be converted to an open approach.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}