
How to Place an Access Port
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS, and Daniel B. Jones, MD, MS, FACS
This month’s technique: Adjustable Gastric Banding: Part 2—How to Place an Access Port
This Month’s Featured Experts:
Jaime Ponce, MD, FACS, FASMBS, Director of Bariatric Surgery, Hamilton Medical Center, Dalton, Georgia; Co-Director of Bariatric Surgery, Memorial Hospital, Chattanooga, Tennesee
Co-Author
Brooke Lindsey, RN, CBN, Bariatric Surgery Clinical Coordinator, Dalton Surgical Group, Dalton, Georgia
Bariatric Times. 2012;9(4):8
Access port placement
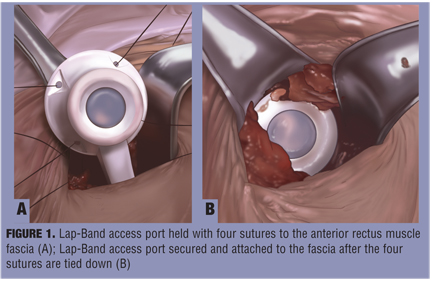
After the tubing is retrieved through the 15mm trocar and delivered into the field, all trocars and the liver retractor are removed. With the Lap-Band (Allergan Inc., Irvine, California), the tubing tab is excised and the tubing is connected to the access port via a metal connector. The tubing should be kept long so that it lies loose within the peritoneal cavity. It is not necessary to close the 15mm trocar site. The access port is secured to the anterior rectus sheath with four nonabsorbable sutures (Figure 1). Exposure of the anterior fascia in a deep abdominal wall can be challenging but is best achieved with the use of deep, narrow Richardson retractors. Four sutures are placed firmly into the sheath and threaded through the four corner holes of the access port. It is important to place the access port at a location distal to the exit point of the tubing to allow a smooth curve into the abdominal cavity.
Mechanical port fixation
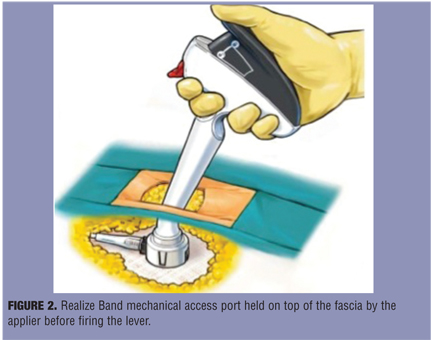
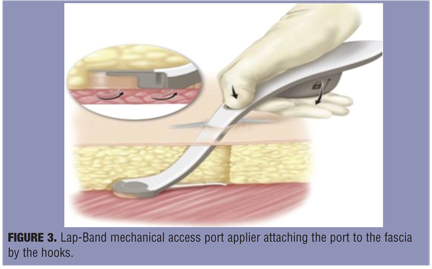
The mechanical port fixation is available for both band brands (i.e., Realize Band, Ethicon Endosurgery, Cincinnati, Ohio [Figure 2] and Lap-Band, Allergan Inc. [Figure 3]). In the mechanical port fixation method the incision is expanded to 4cm to contain the length of the port applier. Fat is dissected away from the fascia on the anterior rectus sheath. The locking connecter of the port is placed around the band tubing with the tubing snug against the port housing. This port has fastening hooks that will attach to the fascia. The port snaps into the applier and the applier is grasped in the palm and inserted into the incision at an angle so that the port base lies uniformly flat on the fascia. The applier’s safety trigger is released, the palm compresses the applier firing lever, and the port is fixed to the fascia. To release the port from the applier, the firing lever must remain compressed as the applier is pulled away. It is important to verify appropriate fascia attachment by the hooks. If proper mechanical fixation cannot be attained, the port should be secured with sutures by way of the holes in the actuator ring or port.
Summary
The system is assembled and the port for inflation and deflation of the band is secured onto the rectus fascia of the anterior abdominal wall. The system is assembled and the port for inflation and deflation of the band is secured onto the rectus fascia of the anterior abdominal wall. Proper port placement is essential for easy access. Adjustment of the band through the access port is an essential part of laparoscopic adjustable gastric banding technique. Appropriate and initially frequent adjustments are critical for successful outcomes
Funding: There was no funding for the preparation of this manuscript.
Disclosures: Dr. Ponce has been a consultant, proctor, and faculty member and has received research support from Allergan and Ethicon Endosurgery, Inc. Ms. Lindsey reports no conflicts of interest relevant to the content of this article.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}