
Laparoscopic Roux-En-Y Fistulo-jejunostomy as a Salvage Procedure in Patients with Persistent Post-Sleeve Gastrectomy Fistula
by Haya Khalfan, MD; Antoine Younan, MD; Georges Khoury, MD; Michel Achkar, MD; and
Elie K. Chouillard, MD, PhD
Haya Khalfan, MD, and Elie K. Chouillard, MD, are from the Division of Bariatric Surgery, Department of Surgery, Poissy/Saint-Germain Medical Center, Poissy, France; Antoine Younan, MD, is from the Department of General Surgery, Bellevue Medical Center, Beirut, Lebanon; Georges Khoury, MD, is from the Department of General and Digestive Surgery, Rizk Medical Center, Beirut, Lebanon; Michel Achkar, MD, is from the Department of Gatrointestinal Endoscopy, Bellevue Medical Center, Beirut, Lebanon.
Bariatric Times. 2014;11(6):8–10.
ABSTRACT
Background: Sleeve gastrectomy is currently the most common bariatric procedure performed in France. It achieves both adequate excess weight loss and significant reduction of comorbidities. Leak, the most common complication after sleeve gastrectomy, has an incidence of less than three percent in specialized centers. Management of leaks after sleeve gastrectomy is difficult and still not standardized. Although preferentially endoscopic and nonoperative, the management of post-sleeve gastrectomy fistulas could eventually be surgical, including peritoneal lavage, abscess drainage, suturing of disrupted staple line, re-sleeve, gastric bypass, or total gastrectomy. Roux-en-Y fistulo-jejunostomy has been described as a salvage option, with only scarce case reports published. Methods: Prior to surgery, intra-abdominal or thoracic collections were treated by computerized tomography scan-guided drainage or surgery and endoscopic stenting was attempted. After optimization of the nutritional status and in cases of failure of conservative measures, Roux-en-Y fistulo-jejunostomy was performed. The technical aspects of Roux-en-Y fistulojejunostomy are discussed. Most procedures were performed laparoscopically. Conclusion: Roux-en-Y fistulo-jejunostomy shoud be considered as a salvage procedure for the treatment of patients with persistent and chronic post-sleeve gastrectomy fistula.
Introduction
Sleeve gastrectomy (SG) is a common treatment for patients with morbid obesity. Initially proposed in patients with superobesity as a first step1 before a more complex procedure (e.g., duodenal switch), SG has become a standard primary procedure2 that can be performed on almost any patient with morbid obesity.
Leak is still the most problematic complication after SG, occurring in up to seven percent of cases in some major series.[3] The management of post-SG fistula is long and cumbersome, especially for leaks located at the esophagogastric junction. In patients with early fistulas presenting with hemodynamic instability, reoperation and repair could be indicated.[4] On the other hand, stable patients with acute fistulas could be managed conservatively (i.e., percutaneous drainage, parenteral or enteral nutrition, proton pump inhibitors, and broad spectrum antibiotics). Finally, if the fistula persists, different options have been proposed, including radiology-guided collection drainage and endoscopy-based treatment (e.g., stents). The goal is to create a temporary “bypass” of the fistula until healing and closure occur spontaneously.
The success rate of such conservative managenent is between 40 and 70 percent.[3]
Patients with persistent fistula are candidates for salvage surgery, including conversion to gastric bypass, or total gastrectomy. In this report, we detail our technique of Roux-en-Y fistulo-jejunostomy (RYFJ)[5] as a salvage procedure for post-SG fistulas resistent to nonoperative treatement.
Technique
The patient is placed in the lithotomy position. Laparoscopy should always be attempted, even in patients with previous laparotomy. The surgeon is positioned inbetween the inferior limbs; the first assistant to the left side and the second assistant to the right side.
The monitor is placed toward the head of the patient on the left side. Under general anesthesia, a 30-degree laparoscope is introduced through a 12-mm incision located 1.5cm to the left side of the midline and 18cm from the xiphoid appendix. Three or four additional trocars, either 5- or 12mm-diameter, are inserted in the upper quadrants, the epigastric area, and the left lateral quadrant, respectively.
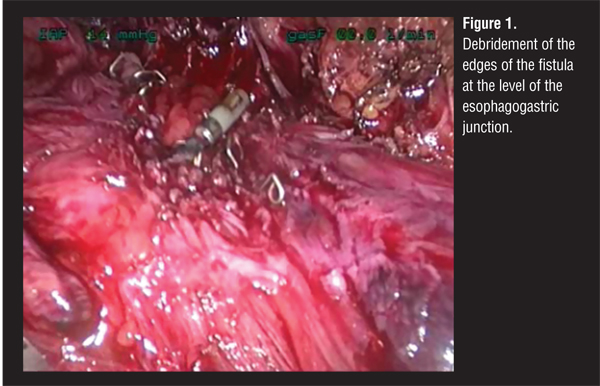
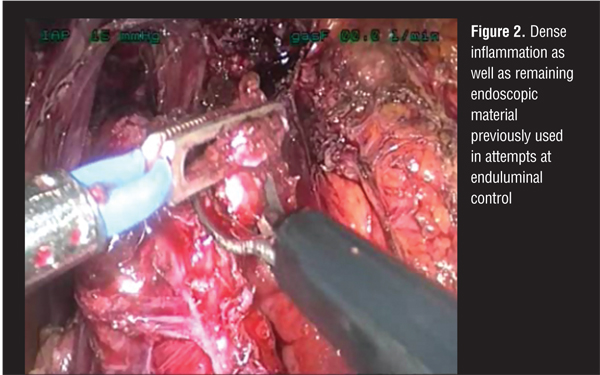
The dissection begins by freeing of the left liver lobe, which is usually very affected by the inflammatory process beneath. Complete dissection of the sleeved stomach is performed, isolating the fistula itself (Figure 1), after removing any material previously used for attempts at endoscopic control (Figure 2). In case of previous percutaneous drainage, the drain tract could be used in order to reach the fistula, avoiding inadvertent tissue damage. It is recommended to use previously nondissected planes, including the pars flaccida, the right crux, and the lesser sac. Every effort should be made to avoid damaging the remaining gastric blood supply (i.e., the right and left gastric arteries). Complete dissection of the esophagogastric junction with mobilization of the lower third of the esophagus is mandatory. This enables tension-free anastomosis between the fistula site and the jejunum, especially in very high fistulas. In case of associated diaphragmatic defects, closure with interrupted nonabsorbable sutures is performed (Figure 3).
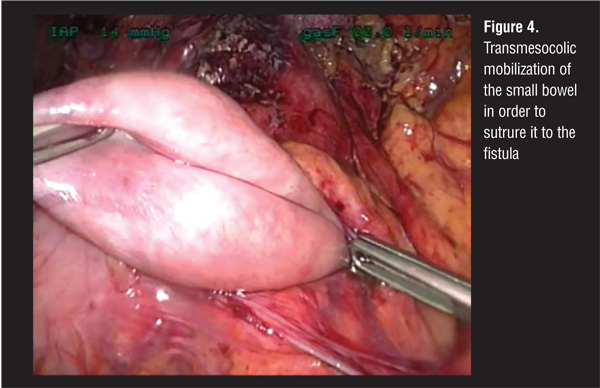
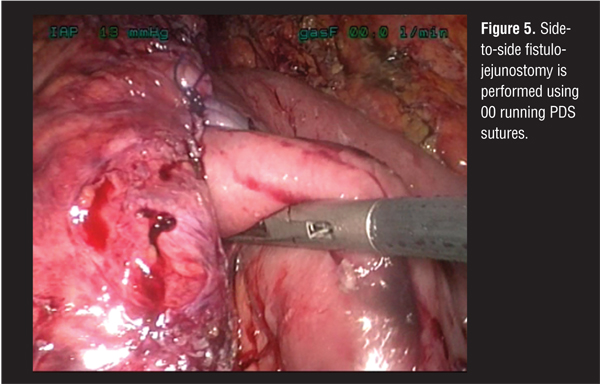
Debridement of the fistula margins is important in order to perform the fistulo-jejunostomy using well vascularized, healthy tissue. The jejunum is then divided 60cm from the Treitz angle and mobilized through the transverse mesocolon (Figure 4). Fistulo-jejunostomy is performed using 00 or 000 PDS running sutures (Figure 5). Jejunojejunostomy is performed using automatic stapling.
The mesocolon defect is closed around the Roux limb using nonabsorbable 00 sutures. Percutaneous closed drainage of the hiatal area is performed. A nasogastric tube with mild negative pressure is left for four days.
In the postoperative period, patients should be kept on parenteral nutrition for seven days. On Day 8 computed tomography (CT) scan with oral contrast fluid should be performed before resuming oral intake.
Upon discharge, patients are prescribed protein pump inhibitors for six months. Additional metabolic or vitamin support is prescribed if required according to specific blood tests.
The patients are re-examined at POD 30 with a CT scan in order to rule out residual fluid collection or fistula.
Long-term multidisciplinary follow-up is similar to that of any patient with bariatric surgery. The patient is evaluated clinically and biologically every three months for two years and then every six months for three years. Blood tests include liver function assessment, Vitamins (B1, B6, B9, B12, D, K), electrolytes, lipids, and thyroid and parathyroid function parameters.
Discussion
Most leaks after SG occur in the proximal third of the stomach, close to the gastroesophageal junction. In our experience, all leaks that were resistant to conservative magaement were located at the gastroesophageal junction. Such fistulas are more likely to occur in SG patients with distal stenosis, resulting in difficulties in gastric emptying. High intraluminal pressure and low compliance of the gastric tube may be the main cause of leak, or even the primum movens in its genesis.[6] Fistulo-jejunostomy seems to be a pathophysiologically relevent solution since it bypasses both difficulties (i.e., gastric lack of compliance and endoluminal high pressure). However, additional factors are most probably implicated in the occurence of fistulas, including impaired suture line healing, poor blood flow, infection, and poor oxygenation with subsequent ischemia.
In our group, the rate of success of endoscopic manegement is over 70 percent with options including biological glues, transoral abscess drainage, and flexible coated stents.[7] Patients who do not respond to endoscopic management and those with recurrent or chronic fistulas are usually candidates for conversion to Roux-en-Y gastric bypass (RYGB) or total gastrectomy. RYGB may be an option in case of possible gastric remnant; however, limitations include the risk of leaving the fistula tract in very high localization and the metabolic consequences of RYGB. Total gastrectomy is associated with a relatively high risk of complications related to the esophagojejunal anastomosis. Moreover, the long-term nutritional consequences are complicated with weight loss, anemia, and the need to readjust the volume and frequencies of meals. We believe that RYFJ is the optimal option since it manages the fistula site in all cases.
Funding: No funding was provided.
Disclosures: The authors report no conflicts of interest relevant to the content of this article.
References
1. Cottam D, Qureshi FG, Mattar SG, et al. Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity. Surg Endosc. 2006;20:859–863.
2. Felberbauer FX, Langer F, Shakeri-Manesch S, et al. Laparoscopic sleeve gastrectomy as an isolated bariatric procedure: intermediate-term results from a large series in three Austrian centers. Obes Surg. 2008;18:814–818.
3. Aurora AR, Khaitan L, Saber AA. Sleeve gastrectomy and the risk of leak: a systematic analysis of 4,888 patients. Surg Endosc. 2012;26:1509–1515.
4. Burgos AM, Braghetto I, Csendes A, et al. Gastric leak after laparoscopic-sleeve gastrectomy for obesity. Obes Surg. 2009;19:1672–1677.
5. Baltasar A, Bou R, Bengochea M, et al. Use of a Roux Limb to correct esophagogastric junction fistulas after sleeve gastrectomy. Obes Surg. 2007;17:1408–1410.
6. Deitel M, Crosby RD, Gagner M. The first International Consensus Summit for Sleeve Gastrectomy (SG), New York City, October 25–27, 2007. Obes Surg. 2008;18:487–496.
7. Tan JT, Kariyawasam S, Wijeratne T, et al. Diagnosis and management of gastric leaks after laparoscopic sleeve gastrectomy for morbid obesity. Obes Surg. 2010;20:403–409.
Category: Brief Report, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}