
Myths Associated with Obesity and Bariatric Surgery
Exclusive Series: The Metabolic Applied Research Strategy Initiative
Bariatric Surgery: Beyond Restriction and Malabsorption
Myth 1: “Weight can be reliably controlled by voluntarily adjusting energy balance through diet and exercise.”
by Lee M. Kaplan, MD, PhD; Randy J. Seeley, PhD; and Jason L. Harris, PhD
Bariatric Times. 2012;9(4):12–13
Abstract
The Metabolic Applied Research Strategy is a multi-year, multi-generational collaborative research program between the Massachusetts General Hospital, the University of Cincinnati, and Ethicon Endo-Surgery. Its focus is to interrogate and understand the physiologic and metabolic changes that occur after bariatric surgery (i.e., how bariatric surgery works to resolve conditions such as type 2 diabetes) with the goal of inventing new, less invasive, and less expensive treatments for patients suffering from obesity and its related health issues. In this article, which is the second in a series of articles published in Bariatric Times dedicated to the Metabolic Applied Research Strategy initiative, the authors discuss past and present understanding on why bariatric surgery works, its true mechanisms of action, and how these findings might help researchers, surgeons, and industry harness the remarkable effectiveness of bariatric surgery.
LEE M. KAPLAN, MD, PhD
Lee M. Kaplan, MD, PhD, is Director of the Obesity, Metabolism & Nutrition Institute at Massachusetts General Hospital (MGH) and Associate Professor of Medicine at Harvard Medical School. He is the Director of the subspecialty Fellowship Program in Obesity Medicine and Nutrition at MGH; Associate Director of the NIH-sponsored Boston-area Obesity and Nutrition Research Center; a member of the NIH Clinical Obesity Research Panel; and past chairman of the Board of the Campaign to End Obesity. Dr. Kaplan’s clinical expertise is in the areas of obesity medicine, gastroenterology, and liver disease. His research program is focused on understanding the mechanisms by which the gastrointestinal tract regulates metabolic function and using physiological and genetic approaches to identify therapeutically relevant subtypes of obesity and its complications.
RANDY J. SEELEY, PhD
Dr. Randy J. Seeley is Professor of Medicine and holds the Donald C. Harrison Endowed Chair at the University of Cincinnati College of Medicine. In 2009, Dr. Seeley was appointed as the Director of the Cincinnati Diabetes and Obesity Center (CDOC). His scientific work has focused on the actions of various peripheral hormones in the central nervous system that serve to regulate food intake, body weight, and the regulation of circulating fuels. In particular, he focuses upon the numerous hypothalamic and gastrointestinal peptides and their associated receptors that influence both energy intake as well as peripheral metabolic processes with the aim of developing new treatment strategies for both obesity and diabetes.
JASON L. HARRIS, PhD
Dr. Jason L. Harris is a Principal Engineer leading Metabolic Applied Research Strategy co-invention and product development efforts at Ethicon Endo-Surgery, a Johnson and Johnson company. Since 2006, he has been exploring novel treatment approaches for patients suffering from the effects of metabolic disease. His primary focus is applying insights from basic and applied research efforts to develop improved therapies and predictive tools for the treatment of this disease.
————
The epidemic of obesity and its medical, sociological, and economic consequences continue to reach further into our society. Its influence touches all specialties of medicine; profoundly affects the quality of life of those affected; and engenders enormous medical, workplace, and personal costs. Obesity has also adversely affected our national security. From 1995 to 2008, the portion of United States military recruits rejected for weight problems jumped from 12 to to 21 percent, even as the prevalence of obesity among military personnel doubled.[1] For the United States population as a whole, the National Bureau of Economic Research (NBER) has estimated that obesity increases annual health care expenses by more than $168 billion,[2] and the Society of Actuaries, which includes lost workplace productivity, estimates the annual cost at closer to $300 billion.[3] For the more than 90 million adults and children with obesity, the consequences are far more severe and include increased likelihood of more than 65 diseases, shortened life expectancy by up to 25 years, inferior quality of life, and exposure to substantial prejudice and stigma. Nearly 1,000 people die each day in the United States from the medical complications of obesity, a rate second only to tobacco as a cause of “preventable” death. So, if obesity is so preventable, why has its prevalence more than doubled in the past 50 years, and why have our efforts to prevent and treat it been so ineffectual?
This article, the second in a series highlighting the Metabolic Applied Research Strategy (MARS) initiative, details some of the frequently cited “myths” surrounding obesity and bariatric surgery, highlighting knowledge gained from MARS and related research efforts across the globe.
Debunking the myth: why weight cannot be reliably controlled by voluntarily adjusting energy balance through diet and exercise
Clinical evidence: long-term failure is the rule. While lifestyle modification remains the mainstay of treatment for obesity and has been shown to be effective in the short term, its ability to provide substantial, durable weight loss is very limited. Among people with established obesity (body mass index [BMI]>30kg/m2), approximately 80 percent will initially lose at least 10 percent of their body weight with a concerted weight loss regimen, but more than 95 percent will regain all of the lost weight (or more) within the subsequent 2 to 5 years. This weight regain has been thought to result from volitional failure of the patient to maintain the regimen that caused the weight loss, but this interpretation overlooks the physiological forces that almost certainly undermine that maintenance.
The regulation of fat mass and, in turn, body weight, require a delicate balance between caloric intake and energy expenditure. To gain one pound over the course of one year (or 45 pounds between the ages of 20 and 65) requires a daily imbalance of just 11 calories. For a person on a diet of 2,500 calories per day, this imbalance represents a mismatch between caloric intake and expenditure of only 0.4 percent. In other words, people who naturally maintain their weight burn 100 percent of ingested calories, while those who are 90 pounds overweight by the age of 65 have burned an average of 99.2 percent—a very small difference in physiology leading to dramatic physical, physiological, and often medical effects. This small mismatch is a minor disturbance of the body’s normal regulatory efficiency, but one that is difficult to overcome.
It is important to note that success is far more likely for those who need to lose only 5 to 15 pounds because the adjustment in physiological set point is so modest. Even so, weight regain and recurrent dieting is usually the norm rather than the exception.
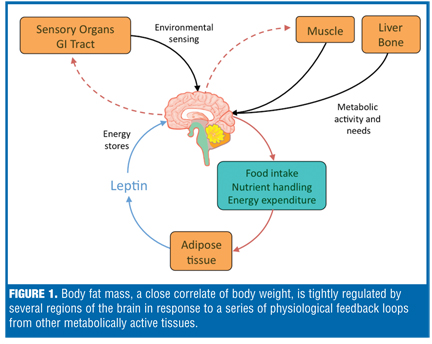
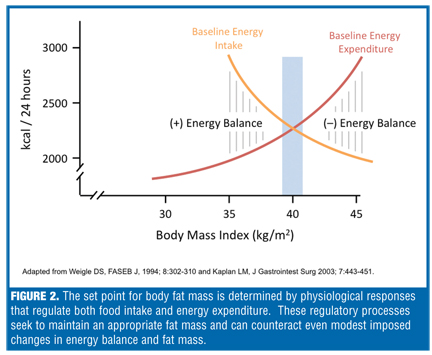
Energy balance is tightly regulated. So, why is it so difficult to lose large amounts of weight and even harder to maintain the weight loss? Among its other functions, body fat is the primary storage depot for energy in the body. We need to maintain appropriate energy stores so that we have adequate reserves both for normal activities and for situations that require additional energy (e.g., infection, illness, injury, increased physical activity), many of which also interfere with acquisition of new energy supplies (eating). As one would expect for any critical metabolic function, the amount of stored energy is highly regulated based on genetic, developmental, and environmental influences. The physiology of body weight regulation is complex (Figure 1) with robust and redundant systems to ensure sufficient, but not excessive, energy stores. Numerous studies in laboratory animals have demonstrated that, even in the presence of infinite food availability, animals regulate their food intake and defend an appropriate fat mass (and consequently, body weight) provided that the available food is “healthy.” This tight regulation of fat mass can be shown in overfeeding or underfeeding studies. Forced alteration of food intake initially has a predictable effect on defended fat mass, with overfeeding causing weight gain and underfeeding causing weight loss. Over time, however, the fat mass and corresponding weight seek a new stable point despite continued overfeeding (e.g., weight gain stops and the weight becomes stable). This happens because physiological changes occur in response to the initial weight gain that cause the animal to increase its total energy expenditure (resting metabolic rate and spontaneous physical activity) in an attempt to shed the excess stored calories. This process of metabolic adaptation also occurs in the setting of food restriction and consequent weight loss. In response to the diet-induced weight loss, metabolic adaptation causes conservation of energy expenditure and stimulation of hunger, both of which help to counteract further weight loss and promote regain of the lost weight, shown in an idealized form in Figure 2. The overall effect of these mechanisms is to defend a stable body fat mass, or energy storage “set point.” Numerous neuro-hormonal mechanisms appear to account for the adaptive response to diet-induced weight change, including increased circulating levels of ghrelin, an appetite-stimulating hormone secreted by the stomach, and decreased levels of peptide YY, cholecystokinin (CCK), glucagon-like peptide 1 (GLP-1), and amylin, hormones that promote satiety and tend to limit food intake. Notably, recent human studies have shown that changes in these hormones are maintained even after prolonged dieting, confirming the findings in animals that even long-term maintenance of lost weight rarely resets the set point.[4] The strength and durability of these physiological mechanisms easily account for the widespread failure of food restriction and enhanced exercise to provide long-term control of obesity.
So, if it’s all about energy storage or body fat “set point,” why do so many of us now have such elevated set points? This, of course, is the key to obesity. Body fat set points appear to be regulated like so many other metabolic and physiological functions in the body, such as blood glucose, LDL cholesterol, blood pressure, and hematocrit. In each case, the “set points” are not firmly fixed; rather, they reflect the integration of genetic predisposition (e.g., some people are just more prone to hypertension), developmental (life) history (e.g., skin color tends to darken, and muscle mass tends to decrease with age), and environmental exposure (e.g., living at high altitudes results in an elevated hematocrit, and medication usage can produce powerful physiological responses). Genetics, developmental history, and environment all contribute to an individual’s set point for body fat mass, but the recent epidemic rise in obesity results primarily from changes in the modern environment leading to an inappropriately elevated set point. Once that elevated set point is established, normal physiological mechanisms defend it. As a result, diet restriction, even modest restriction, can trigger increased hunger and craving, and decreased satiety and conservation of energy expenditure—responses designed to prevent starvation—even in an individual with a BMI that is far from starvation.
Environmental change has increased the set point. There are many changes in the modern environment that appear to promote obesity and its metabolic consequences. Alterations in the chemical and nutrient content of food influence brain physiology through multiple mechanisms (e.g., satiety, palatability, hedonic reward) in ways that affect both food intake and fat mass set point. These changes in our more highly engineered food supply include but are not limited to antibiotics and other chemicals. Lack of exercise changes muscle physiology in ways that appear to promote increased food intake and preference for less healthy varieties. Chronic stress, personal distress, and disruption of sleep and circadian rhythms all promote obesity and metabolic dysfunction. And the widespread use of medications that promote weight gain add to these effects. The net result is a pathophysiological adjustment of the set point that often continues to rise over time.
Need to adjust physiological set point, not only calories in or out. We have learned from clinical observation and carefully controlled studies in animal models that merely contesting the defense of set point is rarely a productive strategy. The key to successful treatment of obesity appears to be in changing the physiological set point back toward a healthier weight, a process that is promoted by a return to healthier, more natural and complex foods, improved muscle function (through regular exercise), stress reduction, improved sleep and circadian patterns, and avoidance of weight-promoting drugs. For effective weight loss, the number of calories ingested needs to decrease and the number of calories burned needs to increase. For long-term success, however, these changes need to be mediated by the normal regulatory processes rather than imposed by voluntary will in an attempt to counteract those processes. Indeed, when the willful actions contradict the physiology, the physiology almost always wins.
Unfortunately for many if not most people with severe obesity, the effects of these environmental and lifestyle changes are not adequate in providing optimal long-term weight loss or reduction in the clinical and psychosocial complications of obesity. This is where surgery can be most helpful. As will be discussed in the next article in this series, many bariatric surgical procedures exert profound effects on fat mass set point, driving down body weight through their direct effects on the regulation of energy balance and metabolic function. These profound physiological effects on fat mass, glucose homeostasis, lipid biology, and many other metabolic functions have given rise to the concept and the growing discipline of metabolic surgery.
References
1. W Christeson, AD Taggart, S Messner-Zidell. “Too fat to fight: retired military leaders want junk food out of America’s schools. Mission: Readiness. 2010. http://cdn.missionreadiness.org/
MR_Too_Fat_to_Fight-1.pdf Accessed April 10, 2012.
2. J Cawley, C Meyerhoefer. The Medical Care Costs of Obesity: An Instrumental Variables Approach.NBER Working Paper No. 16467 2010 Oct.
3. D Behan, S Cox. “Obesity and its relation to mortality and morbidity costs.” Society of Actuaries. December 2010. http://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCMQFjAA&url=http%3A%2F%2Fwww.soa.org%2FWorkarea%2FDownloadAsset.aspx%3Fid%3D30063&ei=5HCMT4uwKuS10QHXnpCIDA&usg=AFQjCNHyLxMzO9hC6p2iE_VZwpkneqjSvw&sig2=GpsGxXYZ1VLL8_iCvygu2Q. Accessed April 10, 2012.
4. P Sumithran, LA Prendergast, E Delbridge, K Purcell, A Shulkes, A Kriketos, J Proietto. Long-term persistence of hormonal adaptations to weight loss. N Engl J Med. 2011;365(17):1597–604.
FUNDING: No funding was provided.
DISCLOSURES: Dr. Kaplan has received research support from the National Institute of Diabetes and Digestive and Kidney Diseases (NIH), Ethicon Endo-Surgery, Merck Research Laboratories, and GI Dynamics. He has done consulting for C.R. Bard, Gelesis, Rhythm Pharmaceuticals, Medtronic, Sanofi-Aventis, Amylin Pharmaceuticals, Allergan, Merck, GI Dynamics, and Johnson & Johnson. Dr. Seeley has received research support, has done speaking or consulting for the following companies: Amylin Pharmaceuticals, Eli Lilly, Johnson & Johnson, Novo Nordisk, Zafgen Inc., Merck, Roche, Alkermes, and Pfizer. Dr. Harris is an employee of Ethicon Endo-Surgery.
Category: MARS Initiative Series, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}