
Noninsulinoma Pancreatogenous Hypoglycemia after Roux-en-Y Gastric Bypass: A More Simple Operative Treatment
Surgical Pearls: Techniques in Bariatric Surgery
Column Editors: Raul J. Rosenthal, MD, FACS, FASMBS and Daniel B. Jones, MD, MS, FACS
This month’s technique: Noninsulinoma Pancreatogenous Hypoglycemia after Roux-en-Y Gastric Bypass:
A More Simple Operative Treatment
This Month’s Featured Expert: Michael G. Sarr, MD
Dr. Sarr is Professor of Surgery, Division of Gastroenterologic and General Surgery, Gastrointestinal Research Unit (GU 10-01), Mayo Clinic, Rochester, Minnesota
Bariatric Times. 2011;8(10):8–9
Introduction
The development of documented, severe hypoglycemic episodes after a Roux-en-Y gastric bypass (RYGB), albeit quite rare (<1%),[1,2] has become a neuroglycopenic syndrome that is of considerable interest to bariatric surgeons, bariatricians, and endocrinologists alike. It is called the noninsulinoma pancreatogenous hypoglycemia syndrome (NIPHS).[3,4]
History
One might ask why we did not see this “syndrome” before the introduction of RYGB. I will maintain that, indeed, we and especially our grey beards from the gastrectomy era (1940s–1980s) have had experience (in retrospect) with a similar side effect of the duodenal bypass obligated by gastrectomies with Roux-en-Y reconstruction. Back then, however, the number of patients at risk was considerably less than the number of patients undergoing RYGB currently.
The spectrum of symptoms was called reactive hypoglycemia, a syndrome seen all too often with the dumping syndrome. Many physicians and surgeons alike have lumped dumping syndrome and reactive hypoglycemia together, thereby overlooking the difference in time of onset of symptoms between these two syndromes that follow restoration of gastrointestinal continuity after gastrectomy (or gastric bypass) by a Roux-en-Y reconstruction.[3]
Moreover, the current interest in the duodenopancreatic (hormonal) axis has increased the interest and the debate over the role of the proximal-most small bowel in control of glucose metabolism, the “incretin concept” of insulin release, and obesity itself. Currently, this control of glucose metabolism remains controversial and of considerable interest. There are still many unanswered questions, such as the following:
1. Should the bariatric surgeon “bypass” the duodenum and if so, how much should be bypassed?
2. Is a limited duodenal bypass appropriate for patients with type 2 diabetes mellitus (T2DM) with only mild-to-moderate obesity?
3. What about for the patient with moderate obesity?
4. Does duodenal bypass contribute to the weight loss independent of caloric intake?
These concerns bring us to the ultimate question—How should we treat the patient who develops severe neuroglycopenic symptoms after RYGB?
First, of course, we must exclude the rare patient with an insulinoma.5 Thereafter, all attempts at nonoperative dietary therapy, such as avoiding high-glucose-dense foods and even pharmacologic therapy (e.g., diazoxide, calcium channel blockers, acarbose)[l,6–8] should be considered and evaluated. But some patients defy all these attempts at nonoperative management, the symptoms are recalcitrant and the neuroglycopenic symptoms are prevalent, dangerous, and even potentially life threatening. When this is the case, some form of definitive operative correction is usually necessary.
Prior suggestions for operative correction have focused on the pancreas as the offending organ with pancreatic islet dysfunction and have involved subtotal pancreatectomy,2 but results have not been successful regarding routine longer-term followup.[3,9] Other surgeons reverted to restoration of normal esophagogastroduodenal anatomy (i.e., takedown of the RYGB),[10,11] and still others have anecdotally evaluated conversion to sleeve gastrectomy.[10,12,13] The goal of these latter procedures is to restore flow of ingested chyme back into the duodenum with the hopes that the reactive overactivity of the islets in the pancreas will resolve (eventually). Reports of these procedures are limited,[10] and long-term follow up concerning overall success and the timeline of resolution of hypoglycemic symptoms are lacking.
At the Mayo Clinic in Rochester, Minnesota, my colleagues and I encountered a patient with severe neuroglycopenic symptoms after a RYGB who had failed nonoperative treatment. The dilemma in this patient was that she had already undergone a revision of her original RYGB that included a gastrectomy of the bypassed stomach, and therefore, was not a candidate for restoration of normal esophagogastroduodenal anatomy nor for conversion to a sleeve gastrectomy. Or was she?
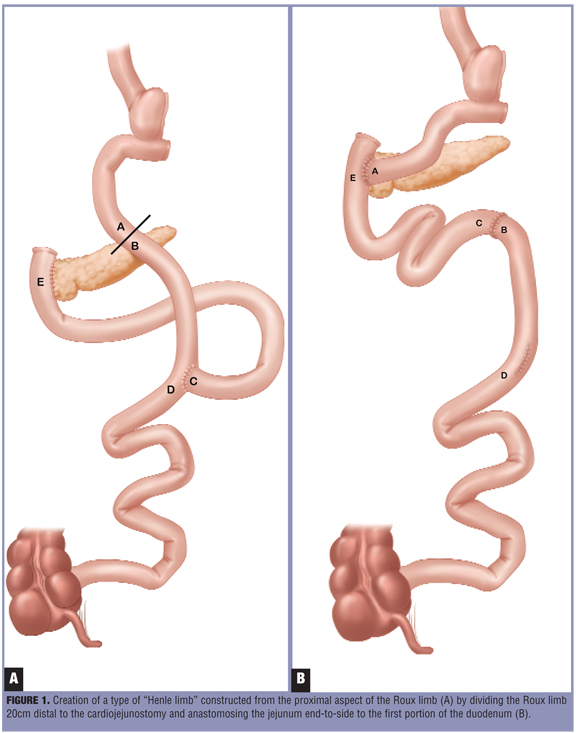
We reasoned that the best way to correct the reactive hypoglycemia was to restore the flow of ingested nutrients into the duodenum. To accomplish this goal, we created a type of “Henle limb” constructed from the proximal aspect of the Roux limb by dividing the Roux limb 20cm distal to the cardiojejunostomy and anastomosing the jejunum end-to-side to the first portion of the duodenum (Figure 1) (i.e., a conduit from a cardiojejunoduodenostomy). To avoid a segment of defunctionalized jejunum, we took down the jejunojejunostomy and anastomosed the distal end of the original pancreatobiliary limb to the distal part of the transected Roux limb, thereby recovering full intestinal continuity. This operative procedure preserved a weight-loss anatomy, as the patient did not want to regain weight, and restored flow of ingested food through the duodenum by an isolated, isoperistaltic jejunal limb (Henle limb). In addition, a jejunal feeding tube was placed as well to provide another potential therapeutic option to treat episodic hypoglycemia. This procedure was a fairly simple, low-risk operation.
At follow up four months postoperatively, her glycopenic symptoms gradually improved markedly (although not totally disappeared) and she did not gain weight. Long-term follow up will be necessary.
Surprisingly and to the best of this author’s knowledge, this simple operation has not been described previously. Restoration of duodenal flow of ingested nutrients has been the goal of prior described operations in an attempt to reverse the reactive hypoglycemia; reported results (all anecdotal) have been encouraging. Conversion to a sleeve gastrectomy has been considered in an attempt to maintain a bariatric anatomy. Our described procedure accomplishes the same goal of restoration of duodenal flow of ingested nutrients but is technically much easier and safer than taking down the prior gastrojejunostomy, doing a gastrogastrostomy, and then resecting the greater curvature side of the stomach to create the “sleeve.” In treating this patient, we decided to use the proximal aspect of the Roux limb as the “sleeve,” (i.e., a Henle limb).
This same procedure can be done in patients with the typical RYGB, and the “bypassed stomach” can remain intact and in situ.
In summary, for patients requiring operative “correction” of NIPHS after RYGB, using the proximal 20cm of the existing Roux limb to divert the ingested food back into the proximal duodenum should in theory reverse (over time) NIPHS. But one must be patient, because the reversal of the pancreatic islet dysfunction likely takes a significant amount of time. This procedure is faster and is technically much easier and safer than conversion to a sleeve gastrectomy or a subtotal pancreatectomy. Moreover, this procedure preserves a bariatric anatomy similar functionally to a sleeve gastrectomy.
References
1. Kellog TA, Bantle JP, Leslie DB, et al. Postgastric bypass hyperinsulinemic hypoglycemia syndrome: characterization and response to a modified diet. Surg Obes Relat Dis. 2008;4:492–499.
2. Marsk R, Jonas E, Rasmussen F, et al. Nationwide cohort study of post-gastric bypass hypoglycemia including 5,040 patients undergoing surgery for obesity in 1986–2006 in Sweden. Diabetologia. 2010; 53:2307–2311.
3. Service FJ, Natt N, Thompson GB, et al. Noninsulinoma pancreatogenous hypoglycemia: a novel syndrome of hyperinsulinemic hypoglycemia in adults independent of mutations in Kir6.2 and SURl genes. J Clin Endocrinol Metab. 1999;84:1582–1589.
4. Service GJ, Thompson FJ, Service FJ, et al. Hyperinsulinemic hypoglycemia with nesidioblastosis after gastric bypass surgery. N Engl J Med. 2005;353(3):249–254.
5. Zagury L, Moreira RO, Guedes EP, et al. Insulinoma misdiagnosed as dumping syndrome after bariatric surgery. Obes Surg. 2004;14:120–123.
6. Won, JGS, Hsaio-Shan T, Yang A, et al. Clinical features and morphological characterization of 10 patients with noninsulinoma pancreatogenous hypoglycaemia syndrome (NIPHS). Clin Endocrinol (Oxf). 2006;65(5):566–578.
7. Gonzalez-Gonzalez A, Delgado M, Fraga-Fuentes M. Use of diazoxide in management of severe postprandial hypoglycemia in patient after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2011 May 27. [Epub ahead of print]
8. Bernard B, Kline GA, Service FJ. Hypoglycaemia following upper gastrointestinal surgery: case report and review of the literature. BMC Gastroenterol. 2010;10:77.
9. Mathavan VK, Arregui M, Davis C, et al. Management of postgastric bypass noninsulinoma pancreatogenous hypoglycemia. Surg Endosc. 2010;24:2547–2555.
10. Cui Y, Elahi O, Andersen OK. Advances in the etiology and management of hyperinsulinemic hypoglycemia after Roux-en-Y gastric bypass. J Gastrointest Surg. 2011 Jun 14. [Epub ahead of print]
11. Dapri G, Cadiere GB, Himpens J. Laparoscopic reconversion of Roux-en-Y gastric bypass to original anatomy: technique and preliminary outcomes. Obes Surg. 2011;21(8):1289–1295.
12. Dapri G, Cadiere GB, Himpens J. Laparoscopic conversion of Roux-en-Y gastriC bypass to sleeve gastrectomy as first step of duodenalswitch: Technique and preliminary outcomes. Obes Surg 2011;21(4):517–523.
13. Personal Communication, Dr. Sayeed Ikramuddin, University of Minnesota.
Category: Past Articles, Surgical Pearls: Techniques in Bariatric Surgery
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
How do I get rid of the LapBand ad overlying the articles?
It is likely your browser window simply needs to be expanded. Click and drag on the bottom right corner of your browser window down and to the right. This should do the trick.