
Pregnancy in Patients with Obesity or Morbid Obesity: Obstetric and Anesthetic Implications
by Anasuya Vasudevan MD, FRCA
Dr. Vasudevan is from the Department of Anesthesia and Critical Care at Beth Israel Deaconess Medical Center and is an Instructor at Harvard Medical School, Boston, Massachusetts.
Bariatric Times. 2010;7(7):9–13
Abstract
The incidence of obesity in women of child bearing age is on the rise, and is a growing healthcare concern. An elevated body mass index has multiple adverse effects on pregnancy. Obesity adversely impacts female reproduction, the fetus, and the peripartum course. The altered physiology, the clinical implications, and the anesthetic and obstetric management are discussed in this article.
Introduction
Obesity is an epidemic in the United States, and its prevalence is on the rise. The incidence of obesity is higher in women aged at least 20 years than in men of the same age. The prevalence of obesity in women of ages at least 20 years is 30.7 percent in non-Hispanic white, 38.4 percent in the Mexican American women, and 49 percent among non-Hispanic black.[1] Obesity in young women of childbearing age does not appear to be on the decline and is one of the leading health concerns in adults.
During the entire course of pregnancy, elevated body mass index (BMI) is an independent risk factor for many maternal and fetal comorbidities. Pregnancy in women who are overweight, obese, or morbidly obese is a major health concern.
Defining Obesity and Weight Gain in Pregnancy
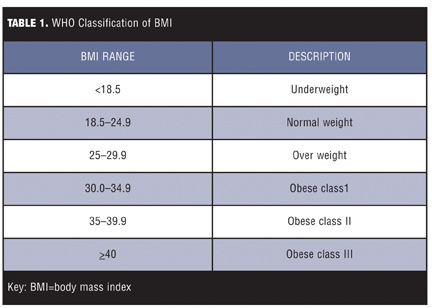
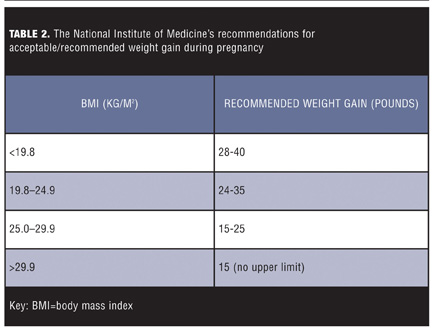
The pre-pregnancy BMI is a reasonable indicator of the severity of obesity. Table 1 shows the World Health Organization (WHO) stratification of BMI. Though pre-pregnancy BMI does not reflect on the pattern of weight gain in pregnancy, it is a valid assessment tool. One of the physiological changes of pregnancy is an increase in body weight. The increase in blood volume, fetus, placenta, amniotic fluid, and increase in body fat stores are some of the factors that contribute to the weight gain. It is essential to recognize that weight gain during pregnancy in women with a normal BMI is different from the allowable weight gain in women with an elevated or low BMI (Table 2).
Higher than recommended weight gain by women who are obese and pregnant results in increased adverse outcomes, such as fetal macrosomia and increased incidence of wound infection.[2,3]
Impact of Obesity on Female Reproduction
Infertility. Obesity is an independent risk factor for infertility. Early onset of obesity in young women can result in irregular menstruation with erratic ovulation. Chronic oligo-ovulation can result in infertility, and the number of women who are obese seeking artificial reproductive technology (ART) is high.[4]
Miscarriage. Metwally et al[5] studied the risk of miscarriage in women who were obese and women who were not obese. Their study included both women who had conceived naturally and those who had required ART. The meta analyses suggest that women with a BMI greater than 25 have a 1.65-fold increased risk for a miscarriage before 20 weeks of gestation. Whether obesity causes more miscarriages in women undergoing ART than natural conception is yet to be determined.[5]
Impact of Obesity on the Fetus
Fetal malformations. A large population-based study from Sweden showed that an elevated pre-pregnancy BMI is associated with a number of congenital defects. The likelihood of neural tube defect, cardiac defects, and orofacial clefts were 4, 1.5, and 1.9 times more in a parturient woman with pre-pregnant morbid obesity.[6] Other investigators have found similar associations. Rasmussen et al[7] found that maternal obesity is associated with a 1.7-fold increase in risk of neural tube defects and with maternal morbid obesity, the risk increased greater than 3-fold.
An abnormality of folate metabolism is speculated to contribute to the high prevalence of neural tube defects in the fetus of the parturient woman with morbid obesity. Werler et al[8] found that despite folate supplementation of 400µcg, women who weighed 70kg or more had consistently low serum folate levels. This suggests the dose of folate supplements in parturient women who are obese should be increased. Despite this association, the authors caution against changing the folate dose in women who are obese until further stronger evidence becomes available.[6,8]
Stillbirth. The risk of stillbirths and intrauterine fetal demise are increased in parturient women who are obese. This association is strong, even when controlling for comorbidities, such as hypertension and diabetes. The increased incidence of stillbirth in parturient women who are obese could be a complication from possible placental insufficiency.[9]
Fetal imaging. Parturient women who are obese are at increased risk for fetal anomaly. The abdominal fat often limits the ultrasound examinations of the fetus. The structures less well seen on ultrasound of women with increasing BMI are fetal heart, spine, kidneys, diaphragm, and umbilical cord. Although improved fetal imaging with advanced ultrasound equipment at a later gestational age may offer better visualization, abdominal fat can still hinder accurate evaluation.[10]
Fetal macrosomia. Fetal macrosomia increases the risk of shoulder dystocia, clavicle fractures, nerve injuries, birth asphyxia, and depressed five-minute Apgar scores and result in increased admission to new born nurseries. Neonates of women who are obese or morbidly obese are at a higher risk of experiencing metabolic abnormalities. The metabolic derangements range from hypoglycemia, hyperglycemia, hypothermia, and hyperbilirubinemia.[11] There is a growing body of evidence from developmental origins of health and disease, which leads to the question of whether maternal obesity causes fetal programming and a predisposition to obesity and its associated metabolic issues.[12,13]
Impact of Obesity on the Parturient Woman
Pregnancy and comorbidities. During the course of pregnancy, even women within the normal preconceptual BMI range are at a risk of developing many comorbid conditions, such as gestational diabetes, pregnancy-induced hypertension, thrombosis varicose veins, anemia, and lower-extremity edema. When obesity or morbid obesity is superimposed on pregnancy, the risk of developing a comorbid condition is significantly higher.
Cardiovascular and hypertensive disorders. The blood volume and cardiac output increase in the early first trimester of pregnancy. Cardiac output increases 30 to 35 percent during the first trimester, and during the third trimester and postpartum period, the cardiac output can increase 50 to 70 percent, compared to the pre-pregnant state. Obesity independently increases blood volume and cardiac output. Cardiac output increases by 30–35mL/min for every 100gm of fat tissue.
The peripheral vascular resistance is low during pregnancy due to elevations in progesterone, which has smooth muscle relaxant properties. The progesterone-induced reduction in afterload may not occur to the same extent in a parturient woman who is obese or morbidly obese, as the arterial walls may be less compliant. The combination of increased cardiac output and elevated afterload contributes to left ventricular hypertrophy. The left ventricle of parturient women who are obese was found to be significantly hypertrophic in comparison to their normal cohorts.[14]
Pregnancy-induced hypertension (PIH) is diagnosed in about seven percent of all pregnancies. A 15-year population-based cohort study by Robinson et al[15] shows that relative to women who are not obese, there was one excess case of PIH per 10 women with moderate obesity and one per seven in women who were severely obese. The more severe forms of PIH i.e., HELLP (hemolysis, elevated liver enzymes, low platelets) syndrome was also more frequent in parturient women who are obese.[15]
Supine hypotension syndrome becomes manifest from 18 to 20 weeks gestation. This is more profound in women who are obese as the fat pannus contributes to further pressure on the inferior vena cava in a supine position. Furthermore, effective left uterine displacement may be very hard to achieve due to the extra weight.
Pulmonary disorders. Pregnancy induces a number of changes to pulmonary physiology and mechanics. Early in pregnancy, the alveolar ventilation is increased and pregnant women have a sense of dyspnea. This is attributed to the respiratory stimulant effect of progesterone. As the uterus enlarges, the residual volume and expiratory reserve volume reduce and, by term, the functional residual capacity is 15 to 20 percent below the nonpregnant state. In addition, the oxygen consumption is increased.
Obesity has similar effects on the pulmonary function (i.e., it reduces the functional residual capacity). Surprisingly, when women are pregnant and obese, the reduction in functional residual capacity does not appear to reduce more.[16] However, the work of breathing increases tremendously and the mismatch in oxygen supply and demand is pronounced. Thus, women who are obese and pregnant have minimal to absent pulmonary reserve and are prone to develop hypoxemia easily.
Obstructive sleep apnea (OSA) is frequently associated with obesity. Progesterone is a respiratory stimulant, but despite this, women who are obese and pregnant may have symptomatic OSA. Patients with significant OSA may require continuous positive airway pressure (CPAP) therapy. The fetus may poorly tolerate maternal nocturnal hypoxemia and CPAP therapy will be beneficial to parturient women with OSA.[17]
Gestational diabetes. During pregnancy, the secretion of human placental lactogen, human chorionic gonadotrophin, and steroid hormones increase the resistance of target tissues to insulin. Obesity is an independent risk factor for diabetes even in the nonpregnant state. Therefore, the magnitude of this association is profound in women who are pregnant and overweight or obese. The risk of developing gestational diabetes mellitus (GDM) is about two, four, and eight times higher among overweight, obese, and severely obese women, respectively.[18] The potential adverse effects from GDM are higher risk of adverse infant outcome, higher risk of mother developing diabetes later in life, and higher risk of diabetes and overweight in the child. Fetal macrosomia is common in GDM and this is associated with adverse fetal outcomes.
Gastrointestinal effects. The placenta secretes gastrin and this can increase the gastric secretions. In addition, progesterone with the smooth muscle relaxant effect can lower the gastroesophageal sphincter tone. Parturient women often experience new-onset heart burn, which is a symptom caused by an incompetent lower gastroesophageal sphincter. Obesity is often associated with acid reflux. The residual gastric volume appears to be higher in women who are obese and in labor than women who are in labor and not obese.
Impact of Bariatric Surgery on Female Reproduction
Interval between bariatric surgery and pregnancy. American College of Obstetricians and Gynecology recommends that women should delay conception for 18 months after weight loss surgery to avoid conceiving during the period of rapid weight loss.[19] Speculative risks of earlier conception include preterm delivery, fetal growth restriction, low birth weight, and fetal anomalies (e.g., open neural tube defects) and minimizing the benefits of maximum weight loss. As weight gain is the norm during pregnancy, the maternal benefits from the weight loss surgery may be limited. The retrospective analysis of 52 women by Wax et al[20] showed no significant differences in the pregnancy or neonatal outcomes in women who conceived less than 18 months and more than 18 months after weight loss surgery.[20]
Advantages of pregnancy post-bariatric surgery. Fertility improves with the weight loss that accompanies bariatric surgery. With reasonable weight loss, obesity-related comorbid conditions improve, with a reduction in the maternal and fetal adverse comes. After bariatric surgery, the incidences of GDM and hypertensive disorders are lower than their controls.[21]
Special considerations for pregnancy after bariatric surgery include the following:
• Adjustment of gastric band may be necessary (inadequate weight gain may cause small-for-gestational-age babies)
• Supplementation to avoid deficiencies of iron, folate, calcium and vitamin B12 is essential. Nonsteroidal, anti-inflammatory drugs should be avoided in women with a history of ulcers. Patients may need to be monitored for symptoms and signs of hypoglycemia.
• There are case reports of intussusceptions post-Roux en Y gastric bypass surgery during pregnancy.
Impact of Obesity on Labor and Labor Outcomes
Post-term pregnancies. Post-term pregnancies, or pregnancies that last 42 weeks or more, are common in women with high BMI. Post-term pregnancy is associated with increased neonatal morbidity. In a retrospective study, Caughey et al[22,23] showed that obesity was a modifiable risk factor that increased the risk of post-term pregnancies by nearly 1.5 times. The combination of maternal age 30 to 39 and obesity increased the risk of post-term pregnancies even more.[22,23]
Dystocia. There is evidence to support that uterine contraction in women who are obese may be altered or impaired in comparison with women of normal BMI.[24] Though women who are obese may demonstrate a shorter latent phase, analysis of labor curves showed a dramatic association with arrest of cervical dilatation (i.e., dystocia of labor).[25]
Uterine monitoring. Monitoring contractions and ensuring adequate strength of contractions can be a challenge in women who are obese and in labor. Manual palpations and external tocometry may be unreliable and use of intrauterine pressure catheters can be advantageous. Newer techniques, such as electrohysterography, may become the preferred monitoring method and may be superior to both tocodynamometry and intrauterine pressure assessment.[26]
Fetal monitoring. A large panniculus can hinder consistent and reliable external fetal monitoring; therefore, fetal scalp monitoring may be warranted for reliable intrapartum fetal monitoring.
Operative deliveries. Dietz et al[27] analyzed the risk of caesarean deliveries in women who were overweight, obese, or morbidly obese. They found that the relative risk of Cesarean section was 1.4 (95% CI 1.0–1.8) for women who were overweight, 1.5 (CI 1.1–2.1) for women who were obese, and 3.1 (95% CI 2.3–4.8) for women who were morbidly obese.[27] Obesity also increases the risk of vertical abdominal incisions, excessive blood loss, and wound infections.[28]
Vaginal birth after Cesarean sections (VBAC). Trial of labor is offered to women with one previous Cesarean section. The success of VBAC is quoted to be about 80 percent.[29] Suspected macrosomia, maternal diabetes, multiple gestation, and maternal obesity are not contraindications for offering a trial of labor. The risk of uterine rupture, especially with augmentation of labor, should be discussed with the patient. The incidence of uterine rupture with the use of cervical ripening agents is quite high. Continuous fetal monitoring is considered safe and the ability to proceed with an operative delivery is a prerequisite.[30]
VBAC is successful in only 13.3 percent of women with high BMIs when compared to the success of VBAC in women with normal BMIs.[31] Obstetricians should also keep in mind the fact that decision to delivery time may be longer in women who are obese and morbidly obese. The reason for this is mutifactorial. The longer duration may be due to difficulty in moving the bed and the patient, the establishment of anesthesia, and difficulty with surgical exposure. However, there are no published data to date that compare the difference between the decision to delivery time (decision by obstetrician to deliver via cesarean section ) in the obese versus. the nonobese parturient.
Obstetric anesthesia. There should be early and clear interdisciplinary communication regarding the management of parturient women who are morbidly obese. The obstetrician should be aware of the high risk of failed intubation and more time that may be required to establish regional anesthesia. The anesthesiologist should evaluate parturient women who are obese and have an assessment and anesthetic plan in place. Adequate time to deal with challenging neuraxial placements should be available.
Labor analgesia. Continuous epidural analgesia, patient-controlled epidural analgesia, and combined spinal epidurals are frequently used to deliver safe labor analgesia. The neuraxial technique can be technically challenging in individuals who are obese or morbidly obese.
Lumbar epidural analgesia. In parturient women who are obese or morbidly obese, many factors contribute to the technical difficulties in establishing epidural catheter placements and labor analgesia. Polley et al[32] found an association between increasing BMI and increasing distance of the epidural space from the skin. The average depth of epidural space was 5cm and increased with increasing BMI.[32]
A prospective observational study of 427 pregnant women showed that both the number of needle passes and the time to placement from skin infiltration were increased with inadequate back flexion and failure to palpate bony landmarks. These two factors significantly increased the difficulties in neuraxial techniques. BMI as a single parameter did not predict technical difficulty. The pattern of fat distribution in individuals who are obese can vary and neuraxial techniques can be surprisingly easy in some. The risks of failed epidural catheters appear to be high in younger women with a BMI of greater than 30. It is important to identify the epidural catheters that may fail during Cesarean section and replace them if as required.[33]
Ultrasound guided placement should be considered in challenging neuraxial procedures. It is necessary to confirm the epidural catheter’s ability to provide adequate bilateral analgesia. The epidural catheter should be placed early in labor. If the catheter is ineffective (i.e., it provides only a one-sided block or no anesthetic level), the catheter should be replaced.
Combined spinal epidural analgesia (CSE). In this is technique, the epidural space is first identified with a 17G epidural needle. Then, a spinal needle is passed through the epidural needle (needle through needle technique) until the operator feels a typical ‘crunchy’ texture of the spinal needle entering the subarachnoid space. Clear and free flow of cerebrospinal fluid is identified. Medication is injected into the spinal fluid to establish immediate onset of analgesia or anesthesia. The spinal needle is then removed and an epidural catheter is threaded through the epidural needle. This technique has an advantage of having an immediate onset. The incidence of complications, such as epidural failures and unintended dural puncture, appear to be lower than with the epidural analgesia alone. We believe that the identification of the subarachnoid space while performing the spinal component of the technique is an additional way to confirm that the epidural needle is in the appropriate location.
With the combined spinal epidural technique, the spinal portion of the technique provides immediate analgesia/anesthesia; therefore, it is not possible to assess the integrity of the epidural catheter immediately. The catheter failure rate following a combined spinal epidural does not appear to be any higher than epidural placement alone.[34]
It is crucial to remember that the risk of epidural catheter failure is high in parturient women who are obese, and the catheter should be taped/secured only after the patient lies down from sitting to lateral decubitus as this reduces the chance for catheter migration out of the epidural space.[35]
Anesthesia for Cesarean sections. Pregnant women have a lower functional residual capacity and increased oxygen consumption. This leads to a reduced oxygen reserve, allowing them to desaturate quickly and profoundly during apneic phases (e.g., as during rapid sequence induction). Adequate preoxygenation is essential, so is acid aspiration prophylaxis and prevention.
It is sensible to calculate induction agents to the lean body mass, and succinylcholine is calculated to the body weight with a maximum of 200mg for a rapid sequence induction.
Regional versus general anesthesia. Even in parturient women who are not obese, regional anesthesia is preferred over general anesthesia. In a retrospective study over a three-year period, Samsoon and Young[36] found the incidence of failed intubation to be 7 out of 1,980 anesthetics in the obstetric population versus the failed intubations in the general surgical population, which were 6 out of 13,380 patients.[36] The risk of failed/difficult intubation and airway complications increases even more in parturient women who are obese or morbidly obese.[37,38] Laryngeal mask airway (LMA) is usually a useful tool in the difficult airway/failed airway algorithm. Unfortunately, this may be less effective in parturient women who are morbidly obese, as higher ventilation pressures are required in the patients who are morbidly obese. Patients who are obese have higher gastric residual volumes, are more likely to have lower esophageal sphincter tone, and have a higher risk for regurgitation of gastric content. LMA ProSeal® (LMA North America, Inc., San Diego, California) has the ability to empty the stomach and has been used to maintain oxygenation in patients with failed intubation for an emergency Cesarean section. However, though LMA ProSeal is a useful tool in the failed airway algorithm, its safety and reliability in maintaining oxygenation in parturient women who are morbidly obese is still anecdotal.[39–41]
If general anesthesia is required for a parturient woman with a potential difficult airway, awake fibreoptic intubation should be considered. Even in emergent situations, the obstetric and anesthesia team need to have clear communication, and if regional anesthesia is deemed feasible, then a spinal anesthesia or continuous spinal anesthesia should be performed. Maternal safety should always be the primary concern. If emergent general anesthesia is deemed necessary (e.g., in a patient with morbid obesity and hemodynamic instability), when induction of general anesthesia seems unavoidable, back up surgical airway should be available.
Labor and delivery suites should have easy access to difficult airway carts and the obstetric anesthesiologist should be proficient with video laryngoscopes and fiberoptic intubations. Video laryngoscopes are proven to improve visualization of the vocal cords in patients with morbid obesity and in patients meeting criteria for predicted difficult intubations.[42,43] Therefore, though there are no published data of the use of video laryngoscopes in pregnant women, they will play an important role in the management of an anticipated difficult intubation.
Spinal anesthesia provides excellent anesthesia for Cesarean section, but the duration of the anesthesia is finite. In patients with morbid obesity, the height of the spinal block may be difficult to predict as the cephalad spread of even epidurally administered bupivacaine is higher than in parturient women who are not obese.[44] This may be due to compression of the thecal sac by the extra weight. Intraoperative conversion to general anesthesia in a parturient woman who is morbidly obese with an unexpected high block or failing regional anesthesia is fraught with complications. There are reports of continuous spinal anesthesia after unintentional dural puncture with an epidural needle. Intrathecal catheters are a reliable way to provide adequate surgical anesthesia. Extra care must be taken to clearly label and communicate with all team members. Mistaking this for an epidural catheter can be fatal, especially in a patient with a difficult airway.
Complications related to neuraxial blocks. The complications related to neuraxial blocks range from failure of the block (e.g., incomplete anesthesia or analgesia), back pain, post-dural puncture headache, and hypotension to permanent nerve damage, epidural abscess, hematoma, and meningitis. Obesity has been identified as a contributory factor for increasing the anesthesia-related complications. The increased incidence of inadequate neuraxial block, multiple attempts at the technique, and higher risk for having the epidural replaced may all contribute to the increased incidence of unplanned dural taps in individuals who are obese. The more severe risks, such as epidural abscess, hematoma, and permanent nerve damage, are extremely rare both in women who are obese and those who are not.[45] There is some evidence, though controversial, that suggests that intrathecal catheters used in patients with obesity leads to a reduction in postdural puncture headaches.[46,47]
Combined spinal epidurals and epidural anesthesia are advocated for Cesarean deliveries. With any regional technique, it is essential to confirm adequate analgesia prior to commencing the surgical procedure. When a combined spinal epidural is performed in a parturient woman who is morbidly obese, it is my practice to administer a small dose of intrathecal drugs. The rest of the anesthesia is established with the epidural catheter. This helps in confirming the functionality of the epidural catheter before the start of the surgery.
It can be catastrophic to perform an urgent intraoperative conversion to a general anesthesia. Inadequate preoxygenation, suboptimal patient position, inadequate access to the patient’s airway, and urgency can all contribute a failed intubation. Maintaining mask ventilation is much harder in a parturient woman with morbid obesity.
Surgery in a parturient women with obesity can be very challenging. Adequate exposure of the lower uterine segment may sometimes require a vertical abdominal incision rather than the transverse pfannensteil incision. Cephalad retraction of the pannus helps with surgical exposure, but there is further compromise of respiratory function with reduction of chest wall compliance. Lifting the pannus off the mother vertically is a better option for both vertical and transverse incisions.
In patients with morbid obesity, airway loss is more frequent at the time of emergence and recovery. Residual effect of anesthetic agents, extubation during Stage 2 of anesthesia, opioids, obstructive sleep apnea, and poor oxygen reserve are the usual contributory factors. Patients with morbid obesity and obstructive sleep apnea or who are at risk for sleep apnea should be monitored closely. Many of the pulmonary complications are averted by having guidelines regarding the post/perioperative management.[48]
Maternal hemorrhage is more common in morbidly obese parturient and blood and blood products should be readily available. The risk of endometritis and wound infection are more frequent in patients with morbid obesity. Parturient women who are morbidly obese are at higher risk for deep vein thrombosis and thrombo embolic phenomenon.[49–51]
Conclusion
Obesity is a rapidly growing pandemic. Adequate prepregnancy counseling and ideal prepregnancy body weight are the best way to improve the outcomes from this disease.[52] Obesity has a multitude of adverse effects on the mother and the fetus. The anesthetic complications can be fatal, and it is essential to have a multidisciplinary management plan that includes the obstetrician, anesthesiologist, and neonatologist to help avoid emergent interventions.
Acknowledgments
I thank Dr. Philip Hess, Director of Obstetric Anesthesia at Beth Israel Deaconess Medical Center, Boston, Massachusetts, for critical appraisal of this manuscript.
References
1. Hedley AA, Ogden CL, Johnson CL, et al. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. JAMA. 2004;291(23):2847–2850.
2. Crane JM, White J, Murphy P, et al. The effect of gestational weight gain by body mass index on maternal and neonatal outcomes. J Obstet Gynaecol Can. 2009;31(1):28–35.
3. Joy S, Istwan N, Rhea D, et al. The impact of maternal obesity on the incidence of adverse pregnancy outcomes in high-risk term pregnancies. Am J Perinatol. 2009;26(5):345–349.
4. Pasquali R, Patton L, Gambineri A. Obesity and infertility. Curr Opin Endocrinol Diabetes Obes. 2007;14(6):482–487.
5. Metwally M, Ong KJ, Ledger WL, Li TC. Does high body mass index increase the risk of miscarriage after spontaneous and assisted conception? A meta-analysis of the evidence. Fertil Steril. 2008;90(3):714–726.
6. Blomberg MI, Kallen B. Maternal obesity and morbid obesity: the risk for birth defects in the offspring. Birth Defects Res A Clin Mol Teratol. 2010;88(1):35–40.
7. Rasmussen SA, Chu SY, Kim SY, et al. Maternal obesity and risk of neural tube defects: a metaanalysis. Am J Obstet Gynecol. 2008;198(6):611–619.
8. Werler MM, Louik C, Shapiro S, Mitchell AA. Prepregnant weight in relation to risk of neural tube defects. JAMA. 1996;275(14):1089–1092.
9. Nohr EA, Bech BH, Davies MJ, et al. Prepregnancy obesity and fetal death: a study within the danish national birth cohort. Obstet Gynecol. 2005;106(2):250–259.
10. Hendler I, Blackwell SC, Bujold E, et al. Suboptimal second-trimester ultrasonographic visualization of the fetal heart in obese women: Should we repeat the examination? J Ultrasound Med. 2005;24(9):1205,1209; quiz 1210–1211.
11. Henriksen T. The macrosomic fetus: a challenge in current obstetrics. Acta Obstet Gynecol Scand. 2008;87(2):134–145.
12. Briese V, Voigt M, Hermanussen M, Wittwer-Backofen U. Morbid obesity: pregnancy risks, birth risks and status of the newborn. Homo. 2010;61(1):64–72.
13. Armitage JA, Poston L, Taylor PD. Developmental origins of obesity and the metabolic syndrome: the role of maternal obesity. Front Horm Res. 2008;36:73–84.
14. Veille JC, Hanson R. Obesity, pregnancy, and left ventricular functioning during the third trimester. Am J Obstet Gynecol. 1994;171(4):980–983.
15. Robinson HE, O’Connell CM, Joseph KS, McLeod NL. Maternal outcomes in pregnancies complicated by obesity. Obstet Gynecol. 2005;106(6):1357–1364.
16. Eng M, Butler J, Bonica JJ. Respiratory function in pregnant obese women. Am J Obstet Gynecol. 1975;123(3):241–245.
17. Roush SF, Bell L. Obstructive sleep apnea in pregnancy. J Am Board Fam Pract. 2004;17(4):292–294.
18. Chu SY, Callaghan WM, Kim SY, et al. Maternal obesity and risk of gestational diabetes mellitus. Diabetes Care. 2007;30(8):2070–2076.
19. American College of Obstetricians and Gynecologists. ACOG committee opinion number 315, September 2005. Obesity in pregnancy. Obstet Gynecol. 2005;106(3):671–675.
20. Wax JR, Cartin A, Wolff R, et al. Pregnancy following gastric bypass for morbid obesity: effect of surgery-to-conception interval on maternal and neonatal outcomes. Obes Surg. 2008;18(12):1517–1521.
21. Abodeely A, Roye GD, Harrington DT, Cioffi WG. Pregnancy outcomes after bariatric surgery: maternal, fetal, and infant implications. Surg Obes Relat Dis. 2008;4(3):464–471.
22. Caughey AB, Stotland NE, Washington AE, Escobar GJ. Who is at risk for prolonged and postterm pregnancy? Am J Obstet Gynecol. 2009;200(6):683.e1,683.e5.
23. Caughey AB, Stotland NE, Washington AE, Escobar GJ. Maternal and obstetric complications of pregnancy are associated with increasing gestational age at term. Am J Obstet Gynecol. 2007;196(2):155.e1,155.e6.
24. Zhang J, Bricker L, Wray S, Quenby S. Poor uterine contractility in obese women. BJOG. 2007;114(3):343–348.
25. Verdiales M, Pacheco C, Cohen WR. The effect of maternal obesity on the course of labor. J Perinat Med. 2009;37(6):651–655.
26. Euliano TY, Nguyen MT, Marossero D, Edwards RK. Monitoring contractions in obese parturients: Electrohysterography compared with traditional monitoring. Obstet Gynecol. 2007;109(5):1136–1140.
27. Dietz PM, Callaghan WM, Morrow B, Cogswell ME. Population-based assessment of the risk of primary Cesarean delivery due to excess prepregnancy weight among nulliparous women delivering term infants. Matern Child Health J. 2005;9(3):237–244.
28. Wall PD, Deucy EE, Glantz JC, Pressman EK. Vertical skin incisions and wound complications in the obese parturient. Obstet Gynecol. 2003;102(5 Pt 1):952–956.
29. Dodd J, Crowther C. Vaginal birth after caesarean versus elective repeat caesarean for women with a single prior caesarean birth: a systematic review of the literature. Aust N Z J Obstet Gynaecol. 2004;44(5):387–391.
30. ACOG Committee on Obstetric Practice. Committee opinion. induction of labor for vaginal birth after Cesarean delivery. Obstet Gynecol. 2002;99(4):679–680.
31. Carroll CS S, Magann EF, Chauhan SP, et al. Vaginal birth after Cesarean section versus elective repeat Cesarean delivery: weight-based outcomes. Am J Obstet Gynecol. 2003;188(6):1516,20; discussion 1520–1522.
32. Clinkscales CP, Greenfield ML, Vanarase M, Polley LS. An observational study of the relationship between lumbar epidural space depth and body mass index in michigan parturients. Int J Obstet Anesth. 2007;16(4):323–327.
33. Orbach-Zinger S, Friedman L, Avramovich A, et al. Risk factors for failure to extend labor epidural analgesia to epidural anesthesia for Cesarean section. Acta Anaesthesiol Scand. 2006;50(8):1014–1018.
34. Norris MC. Are combined spinal-epidural catheters reliable? Int J Obstet Anesth. 2000;9(1):3–6.
35. Hamilton CL, Riley ET, Cohen SE. Changes in the position of epidural catheters associated with patient movement. Anesthesiology. 1997;86(4):778,84; discussion 29A.
36. Samsoon GL, Young JR. Difficult tracheal intubation: a retrospective study. Anaesthesia. 1987;42(5):487–490.
37. Hood DD, Dewan DM. Anesthetic and obstetric outcome in morbidly obese parturients. Anesthesiology. 1993;79(6):1210–1218.
38. Cooper GM, McClure JH. Anaesthesia chapter from saving mothers’ lives: reviewing maternal deaths to make pregnancy safer. Br J Anaesth. 2008;100(1):17–22.
39. Bullingham A. Use of the ProSeal laryngeal mask airway for airway maintenance during emergency caesarean section after failed intubation. Br J Anaesth. 2004;92(6):903; author reply 904.
40. Cook TM, Nolan JP. Failed obstetric tracheal intubation and postoperative respiratory support with the proseal laryngeal mask airway. Anesth Analg. 2005;100(1):290; author reply 290–291.
41. Vaida SJ, Gaitini LA. Another case of use of the ProSeal laryngeal mask airway in a difficult obstetric airway. Br J Anaesth. 2004;92(6):905; author reply 905.
42. Bathory I, Granges JC, Frascarolo P, Magnusson L. Evaluation of the video intubation unit in morbid obese patients. Acta Anaesthesiol Scand. 2010;54(1):55–58.
43. Jungbauer A, Schumann M, Brunkhorst V, et al. Expected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients. Br J Anaesth. 2009;102(4):546–550.
44. Hodgkinson R, Husain FJ. Obesity, gravity, and spread of epidural anesthesia. Anesth Analg. 1981;60(6):421–424.
45. Singh S, Chaudry SY, Phelps AL, Vallejo MC. A 5-year audit of accidental dural punctures, postdural puncture headaches, and failed regional anesthetics at a tertiary-care medical center. Scientific World J. 2009;9:715–22.
46. Faure E, Moreno R, Thisted R. Incidence of postdural puncture headache in morbidly obese parturients. Reg Anesth. 1994;19(5):361–363.
47. Denny NM, Selander DE. Continuous spinal anaesthesia. Br J Anaesth. 1998;81(4):590–597.
48. Gross JB, Bachenberg KL, Benumof JL, et al. Practice guidelines for the perioperative management of patients with obstructive sleep apnea: a report by the american society of anesthesiologists task force on perioperative management of patients with obstructive sleep apnea. Anesthesiology. 2006;104(5):1081,93; quiz 1117–1118.
49. Khashan AS, Kenny LC. The effects of maternal body mass index on pregnancy outcome. Eur J Epidemiol. 2009;24(11):697–705.
50. Schrauwers C, Dekker G. Maternal and perinatal outcome in obese pregnant patients. J Matern Fetal Neonatal Med. 2009;22(3):218–226.
51. Farah N, Maher N, Barry S, et al. Maternal morbid obesity and obstetric outcomes. Obes Facts. 2009;2(6):352–354.
52. Shaikh H, Robinson S, Teoh TG. Management of maternal obesity prior to and during pregnancy. Semin Fetal Neonatal Med. 2010;15(2):77–82.
Funding:
There was no funding for the development of this article.
Financial Disclosures:
The author reports no conflicts of interest relevant to the content of this article.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
There are updated recommendations for weight gain during pregnancy from IOM which were released in May of 2009; including provisional guidelines for women pregnant with twins.
http://www.iom.edu/pregnancyweightgain