
Psychiatric Medications and Weight Gain: A Review
by Thomas Rosko, MD
Dr. Rosko is Director, Psychosomatic Medicine, Department of Psychiatry and Behavioral Neurosciences, Cedars-Sinai Medical Center, Los Angeles, California.
Financial disclosure: Dr. Rosko is on the Speaker’s Bureau for Ortho-McNeil-Janssen Pharmaceuticals and Bristol-Myers Squibb Corporation.
Bariatric Times. 2011;8(3):12–15Abstract
Psychiatric medications, like all medications, are associated with potential adverse effects. One such adverse effect of psychiatric medication is change in body weight. This review summarizes recent evidence and clinical experience in this area and offers suggestions regarding choice of psychiatric agent when weight gain is an important issue.
Introduction
Drugs used to treat psychiatric disorders have numerous potential adverse effects, including weight gain and associated metabolic abnormalities (e.g., glucose intolerance and dyslipidemia). Medication-induced weight gain might also predispose patients to hypertension and cardiovascular disease and make nonadherence with treatment recommendations more likely.
These side effects are especially troublesome for patients with obesity who already suffer from high rates of diabetes and cardiovascular disease. Furthermore, the use of psychiatric medication itself poses particular problems in the population with obesity. Proper medication dosing can be a clinical challenge, especially after bariatric surgery, when medication tablets often must be “crushed and floated” rather than swallowed intact. The bioavailability of crushed medication can differ substantially compared to the same medication swallowed whole, most notably for sustained-release formulations. Crushing a sustained-release tablet can result in very rapid bioavailability of the entire amount of drug in the tablet.
A case report of a patient fatality[1] attributes the death of the patient to this mechanism.
This article will review the potential for weight gain and offer recommendations regarding the use of several major classes of psychiatric medications, including antidepressants, antipsychotics, and mood stabilizers.
Depression and Antidepressants
Depression is a common and serious mental disorder. The prevalence of major depressive disorder (MDD) at any time in community samples is 5 to 9 percent for women and 2 to 3 percent for men; lifetime prevalence is 10 to 25 percent for women and 5 to 12 percent for men.[2]
The World Health Organization (WHO) has used the concept of global burden of disease as a standard metric of well being since 1990. Importantly, this time-based measure includes years of life lost due to living with medical or psychiatric illness (morbidity) as well as years of life lost due to premature mortality. In 2008, depressive disorders were the third leading cause of disease burden worldwide; respiratory infections and diarrheal diseases ranked first and second, respectively. By 2020 the WHO predicts that depression will be the leading cause of disease burden in the world.[3] These statistics represent patients diagnosed with full-blown major depression. Many more patients suffer from “subthreshold depression” or “minor depression” (i.e., clinically significant depressed mood without meeting criteria for MDD).[4]
The relationship between obesity and depression is complex and differs between the sexes. A population study of 40,000 individuals[5] found that men with obesity were less likely to suffer from MDD than their normal weight counterparts. Underweight men, by contrast, were at increased risk for both MDD and suicidal thinking. The same study found the reverse to be true for women. Women with obesity suffered more major depression and suicidal ideation compared to women who were not obese.
Pharmacological agents have become the mainstays of depression treatment. The first antidepressants historically included compounds with a three-ring structure, hence the name “tricyclic antidepressants” (TCA). These include amitriptyline (Elavil), imiprimine (Tofranil), nortriptyline (Pamelor, Aventyl), desipramine (Norpramin), clomipramine (Anafranil), and doxepin (Sinequan).[6] Newer agents, such as the selective serotonin reuptake inhibitors (SSRI), have superseded the use of these medications to treat depression. Nevertheless, clinicians today still use the TCAs for a variety of conditions, including anxiety disorders and neuropathic pain, as well as for depression. Clinicians and their patients have noted the occurrence of weight gain in taking TCAs. One study of pooled data compared the TCA imiprimine with the SSRIs and found a greater incidence of weight gain in patients taking the TCA.[7] Weight gain associated with TCAs tends to be greater with amitriptyline and imiprimine compared to the other drugs in this class.[8]
The SSRIs include fluoxetine (Prozac), sertraline (Zoloft), paroxetine (Paxil), fluvoxamine (Luvox), citalopram (Celexa), and S-citalopram (Lexapro). These medications are widely prescribed to treat depression, anxiety disorders, and other conditions. Initial studies and clinical impressions indicated that these agents did not result in weight gain and, in fact, were more likely to result in mild weight loss, especially with short-term use. In one six-week study, patients taking fluoxetine actually lost weight; the mean weight decrease was 0.84kg.[9] A similar result was noted in a 12-week fluoxetine study; patients lost an average of 0.35kg.[10] Patients with depression treated with the SSRI sertraline in an eight-week study had a mean weight loss of 0.79kg.[11]
In a longer-term study published in 2000, Fava et al[12] at the Massachusetts General Hospital noted that SSRI treatment of patients with MDD is typically not short term; such treatment is commonly continued for at least 4 to 6 months after symptom improvement occurs. They, therefore, compared weight change in patients with depression treated with fluoxetine, sertraline, or paroxetine for 26 to 32 weeks.[12] Significant differences were observed among the three groups in mean weight gain. Fluoxetine patients saw their weight decrease an average of 0.2 percent and sertraline patients gained an average of 1.0 percent. The patients treated with paroxetine, however, experienced an average weight gain of 3.6 percent. Important differences were also noted in the percentage of patients gaining an “extreme” amount of weight—that is, greater than seven percent of body weight. In this study, 25.5 percent of paroxetine patients gained greater than seven percent of body weight compared to 6.8 percent and 4.2 percent of fluoxetine and sertraline patients, respectively.
Another class of antidepressant medications is the serotonin norepinephrine reuptake inhibitors (SNRI). These medications include venlafaxine (Effexor), desvenlafaxine (Pristiq) and duloxetine (Cymbalta). Weight gain is not noted to be a problem with these medications, possibly because their mechanism of action causes an increase in norepinephrine effects. The prescribing information for all three of these drugs cites decreased appetite and weight loss as possible effects.[13–15]
Bupropion (Wellbutrin) is an antidepressant medication with a unique pharmacologic profile.[16] Unlike the drugs previously discussed, bupropion has no effect on the serotonin reuptake transporter. Its mechanism of action appears to result from dopamine and norepinephrine reuptake inhibition (DNRI) with none of its effects mediated by serotonin. It also exhibits no action at the histamine-1 receptor. Perhaps because of this pharmacodynamic profile, patients with depression treated with bupropion typically experience little or no weight gain or even weight loss in both short-term[17] and longer-term[18] studies.
One study[19] evaluated bupropion as a weight loss treatment in outpatients with obesity and depression. All patients were managed with a restricted-calorie diet and received either bupropion or placebo. The bupropion group lost significantly more weight (4.6%) compared to the group treated with diet alone (1.8%). Symptoms of depression were also significantly more improved in the bupropion-treated patients.
Another antidepressant with a distinctive pharmacologic profile is mirtazapine (Remeron). The prescribing information for this agent as well as clinical experience note increased appetite and weight gain as adverse effects.[20] In one study[21] of depressed outpatients, increased appetite occurred in 30 percent and weight gain in 23 percent of subjects. Indeed, clinicians frequently put these “adverse” effects of mirtazapine to good use in patients for whom increased appetite and weight gain are desirable (e.g., anorexic and cachectic patients suffering from human immunodeficiency virus disease or cancer). The pharmacologic effects of mirtazapine are dose related. Increased norepinephrine effects predominate at higher doses, prompting some authors to suggest that mirtazapine’s propensity to cause increased appetite and weight gain might be lessened at doses higher than 15mg per day.[22]
In summary, antidepressant medications have differential effects on body weight. In patients for whom avoiding weight gain is an important consideration, the best antidepressant choices are bupropion or an SNRI, such as venlafaxine, desvenlafaxine, or duloxetine. Mirtazapine, with its typical effect of increased appetite and weight gain, should generally be avoided in these patients.
Bipolar Disorder and Mood Stabilizers
Bipolar I disorder is a chronic and persistent mental disorder that affects about one percent of the general population. As opposed to MDD (called “unipolar” depression by some), patients suffering from bipolar I disorder suffer from mood states that change over time, rapidly and profoundly. In addition to clinically significant depression, these patients experience episodes that are essentially the opposite of depression; that is, they experience periods of elevated, expansive, or irritable mood that cause marked suffering and functional impairment.[23]
Although early studies suggested a greater incidence of obesity in patients with bipolar disorder, more recent studies have shown that the incidence of obesity in patients with bipolar disorder is essentially the same as the incidence of obesity in the general population.[24]
Pharmacological treatment of bipolar disorder is carried out with mood stabilizers including lithium, valproic acid (Depakote), lamotrigine (Lamictal), and topiramate (Topamax). Other classes of medication used to treat these patients include antipsychotics and antidepressants.
Weight gain is commonly seen in patients treated with lithium. One prospective study[25] found weight gain in 74 percent of lithium-treated patients, including a weight increase of 10kg or more in 21 percent. An average weight gain of 10kg or more has been reported in patients on long-term lithium maintenance treatment.[26] Weight gain due to hypothyroidism can also occur in some patients who develop this lithium-related adverse effect.
Valproic acid treatment is often associated with significant weight gain. In one study,[27 23] percent of patients treated with valproic acid gained seven percent or more of body weight. This same study found that patients treated with topiramate consistently lost weight. However, the efficacy of topiramate in treating bipolar patients has not been clearly established.
Lamotrigine, an effective treatment for depression associated with bipolar disorder, is not associated with weight gain.
In summary, the classic mood stabilizers are typically associated with a propensity to gain body weight. An exception is lamotrigine, an agent used to treat bipolar depression. Another class of drugs used to treat bipolar patients is the antipsychotics.
Schizophrenia and Antipsychotic Medications
Schizophrenia is a devastating condition characterized by several different symptom complexes. “Positive” symptoms include hallucinations and delusions. “Negative” symptoms include apathy, anhedonia, and withdrawal from interpersonal contact; much of the impairment and suffering experienced by these patients results from these negative symptoms. Patients with schizophrenia also suffer from abnormal mood states and impaired cognition.
The incidence of obesity in these patients is significantly increased compared to obesity rates in the general population This is especially true of women who suffer from schizophrenia.[28]
Pharmacological treatment remains the cornerstone of patient management. Antipsychotic medications are somewhat misnamed. These drugs are used to treat a variety of conditions, including bipolar disorder, MDD, delirium, dementia, and autism. A useful way to categorize antipsychotic medication is “first generation” or “typical” as opposed to “second generation” or “atypical.” First-generation or typical antipsychotics include chlorpromazine (Thorazine), haloperidol (Haldol), and thioridazine (Mellaril). They are generally associated with less weight gain than the atypical drugs. Two older antipsychotics, loxapine (Loxitane) and molindone (Moban), are associated with little or no weight gain and may result in actual weight loss.[29] These typical antipsychotics were the only drugs available to treat schizophrenia until the availability of atypical agents in the 1990s.
The vast majority of antipsychotic prescriptions today are written for the atypical drugs. These include risperidone (Risperdal), olanzapine (Zyprexa), quetiapine (Seroquel), ziprasidone (Geodon), and aripiprazole (Abilify). A sixth atypical antipsychotic medication is clozapine (Clozaril). Clozapine treatment is characterized by numerous potential adverse effects including rare agranulocytosis; it is reserved for second- or third-line treatment of patients who do not respond to other medications.
A consensus statement on antipsychotic drugs, obesity, and diabetes was published in 2004.30 This paper was written by experts representing four professional organizations: the American Association of Clinical Endocrinologists, the American Diabetes Association, the North American Association for the Study of Obesity, and the American Psychiatric Association. The authors rated the six atypical antipsychotics according to their propensity to cause weight gain. They concluded that the drugs most likely to increase body weight were clozapine and olanzapine. Aripiprazole and ziprasidone were least likely to cause weight gain, with quetiapine and risperidone showing an intermediate effect on weight gain risk. The authors noted that the mechanism(s) by which these drugs cause weight gain is unknown. The atypical antipsychotics exhibit effects at numerous brain receptor sites including those for dopamine, serotonin, histamine, and norepinephrine. It is assumed, but not proved, that weight gain associated with atypicals is somehow related to action at these sites manifesting as increased appetite and/or decreased satiety. Some patients, however, have developed new cases of diabetes while taking olanzapine or clozapine even though they had not gained weight.[31]
The treatment of patients suffering from psychotic illness is a good illustration of the necessity for careful evaluation of risk and benefit whenever psychiatric medication is prescribed. A patient who derives substantial relief from hallucinations and delusions and thinking impairment might be willing to accept greater side effect risk, including risk of weight gain, in return for relief from these debilitating symptoms.
Conclusions
Increased body weight is a potential side effect of some medications used to treat mental disorders. The possibility of weight gain is one factor among many that clinicians must consider in prescribing psychiatric medications. Clinicians should counsel patients regarding the possibility of weight gain and make measurement of body weight, body mass index (BMI), and waist circumference regular aspects of patient care. There are no medications approved by the United States Food and Drug Administration to treat weight gain associated with psychiatric medications. Patients taking these medications might benefit from a proactive approach to weight management that includes nutritional counseling and a program of regular physical exercise.
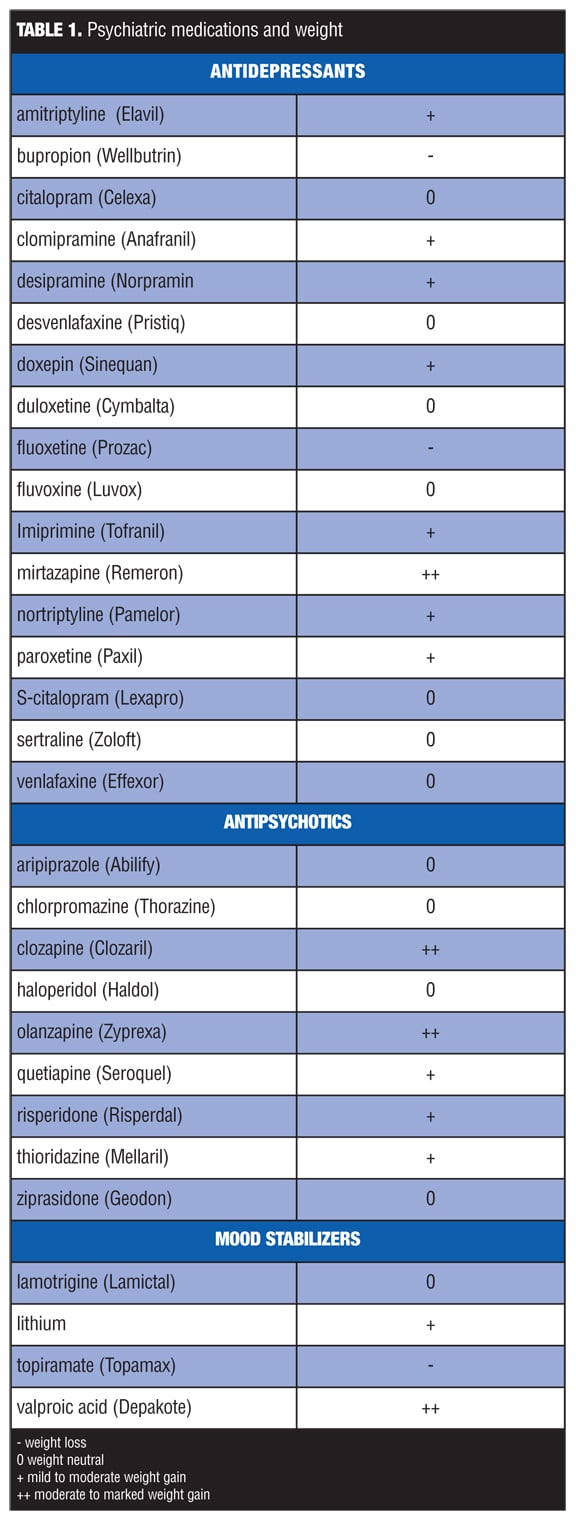
TABLE 1. Psychiatric medications and weight
Acknowledgment
This article is part of a series of articles being published in Bariatric Times that are based on sessions presented at the “Comprehensive Approach to the Treatment of Obesity,” by Cedars-Sinai Medical Center on October 22, 2010.
References
1. Schier JG, Howland MA, Nelson LS, et al. Fatality from administration of labetolol and crushed extended-release nifedipine. Ann Pharmacother. 2003;37(10):1420–1423.
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC:American Psychiatric Association;2000.
3. World Health Organization. Pharmacological treatment of mental disorders in primary health care. 2010. http://www.who.int/mental_health/management/psychotropic/en/index.html. Accessed March 10, 2011.
4. Pincus HA, Davis WW, McQueen LE. Subthreshold mental disorders. A review and synthesis of studies on minor depression and other ‘brand names.’ Br J Psychiatry. 1999;174:288–296.
5. Carpenter KM, Hasin DS, Allison DB, et al. Relationships between obesity and DSM-IV major depressive disorder, suicide ideation, and suicide attempts: results from a general population study. Am J Public Health. 2000; 90:251–257.
6. Schatzberg AF, Nemeroff CB, eds. APPI Textbook of Psychopharmacology, Fourth Edition. Arlington, VA: American Psychiatric Publishing, Inc.;2009.
7. Sussman N, Ginsberg DL, Bikoff J. Effects of nefazodone on body weight: a pooled analysis of selective serotonin reuptake inhibitors and imiprimine controlled trials. J Clin Psychiatry. 2001;62(4):256–260.
8. Berken GH, Weinstein DO, Stern WC. Weight gain. A side effect of tricyclic antidepressants. J Affect Disord. 1984;7(2):133–138.
9. de Jonghe F, Ravelli DP, Tuynman-Qua H. A randomized, double-blind study of fluoxetine and maprotiline in the treatment of major depression. Pharmacopsychiatry. 1991;24:62–67.
10. Michelson D, Amsterdam JD, Quitkin FM, et al. Changes in weight due to a 1-year trial of fluoxetine. Am J Psychiatry. 1999;156:1170–1176.
11. Croft H, Settle EJ, Houser T, et al. A placebo-controlled comparison of the antidepressant efficacy and effects on sexual functioning of sustained-release bupropion and sertraline. Clin Ther. 1999;21:643–658.
12. Fava M, Judge R, Hoog SL, et al. Fluoxetine versus sertraline and paroxetine in major depressive disorder: changes in weight with long-term treatment. J Clin Psychiatry. 2000;61:11:863–867.
13. Effexor Prescribing Information, Pfizer Corporation, Wyeth 2009.
14. Pristiq Prescribing Information, Pfizer Corporation, Wyeth 2010.
15. Cymbalta Prescribing Information, Eli Lilly Corporation, 2008.
16. Schatzberg AF, Nemeroff CB, eds. APPI Textbook of Psychopharmacology, Fourth Edition. Arlington, VA: American Psychiatric Publishing, Inc.;2009.
17. Thase ME, Clayton AH, Haight BR, et al. A double-blind comparison between bupropion XL and venlafaxine XR: sexual functioning, antidepressant efficacy, and tolerability. J Clin Psychopharmacol. 2006; 26:482–488.
18. Croft H, Houser TL, Jamerson BD, et al: Effect on body weight of bupropion sustained-release in patients with major depression treated for 52 weeks. Clin Ther. 2002; 24:662–672.
19. Jain, AK et al. Bupropion SR vs. placebo for weight loss in obese patients with depressive symptoms. Obes Res. 2002; 10(10):1049–1056.
20. Remeron Prescribing Information. Organon International, 1999.
21. Fava M, Dunner DL, Greist JH, et al. Efficacy and safety of mirtazapine in major depressive disorder patients after SSRI treatment failure: an open-label trial. J Clin Psychiatry. 2001; 62:413–420.
22. Fawcett J, Barkin RL. Review of the results from clinical studies on the efficacy, safety and tolerability of mirtazapine for the treatment of patients with major depression. J Affect Disord. 1998;51:267–285.
23. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, DC:American Psychiatric Association; 2000.
24. Hedley, AA, Ogden CL, Johnson, CL, et al: Prevalence of overweight and obesity among US children, adolescents and adults, 1999–2002. JAMA. 2004; 291:2847–2850.
25. Vestegaard P, Poulstrup I, Schou M. Prospective studies on a lithium cohort. Acta Psychiatr. Scand. 1988;78 (4):434–441.
26. Sachs G, Guile C: Weight gain associated with antipsychotic drugs. J Clin Psych. 1999;60 (Suppl 21):16–19.
27. Chengappa KN, Chalasani L, Brar JS, et al. Changes in body weight and body mass index among psychiatric patients receiving lithium, valproate or topiramate. Clin Ther. 2002; 24(10):1576–1584.
28. Allison DB, Fontaine KR, Heo, M et al. The distribution of body mass index among individuals with and without schizophrenia. J Clin Psychiatry. 1999;60:215–220.
29. Stanton JM. Weight gain associated with neuroleptic medication: a review. Schizophr. Bull. 1995;21(3):463–472.
30. Consensus development conference on antipsychotic drugs and obesity and diabetes. Diabetes Care. 2004;27(2):596–601.
31. Wirsching DA, Spelling BJ, Erhart SM, et al. Novel antipsychotics and new onset diabetes. Biol Psych. 1998;44 (8):778–783.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
You reccomend Desveniafaxine yet it is only in extended release form & those aren’t recommended post gastric surgery. What SNRI option is available that is not extended release?