
Single Anastomosis Gastric Bypass in a Patient with Morbid Obesity and Midgut Malrotation
by Ajay H. Bhandarwar, MBBS, MS (Surgery), FMAS, FIAGES, FAIS, FICS, fbms; Chintan B. patel, MS (Surgery), FMAS, FIAGES, fbms; Pravin N. Tungenwar, MS (Surgery), FMAS, FIAGES; Amol N. Wagh, MS (Surgery), FMAS, FIAGES, FICS, fbms; Saurabh S. Gandhi, MS (Surgery), FMAS, FIAGES
Dr. Bhandarwar is a Professor at the Grant Government Medical College & Sir J.J. Group Of Hospitals, in Mumbai, India. Dr. Tungenwar is an Associate Professor at the Grant Government Medical College & Sir J.J. Group Of Hospitals. Drs. Patel, Wagh, and Gandhi are Assistant Professors at the Grant Government Medical College & Sir J.J. Group Of Hospitals.
Bariatric Times. 2015;12(10):12–13.
ABSTRACT
Bariatric surgery has become the treatment of choice for morbid obesity, with the volume of cases increasing steadily. We report a rare case of midgut malrotation in a patient with morbid obesity that was diagnosed during a laparoscopic single anastomosis gastric bypass or “minigastric bypass.” We discuss the challenges of dealing with this intraoperative surprise and the tactics for a safe and successful outcome. This is the first video-documented case of its kind.
Introduction
Obesity is a universal disease, which is increasing in prevalence and is becoming alarmingly epidemic. It is undoubtedly a major public health problem of modern society.[1] Due to lack of effectiveness of conservative treatments, bariatric surgeries currently represent the chosen treatment in cases of morbid obesity, and are performed worldwide.[2–14] With an increasing number of bariatric surgeries, the chances for the surgeon to face unusual anatomical variations, such as intestinal malrotation, also increase.[8] Intestinal malrotations are rare and may be asymptomatic until adulthood. Thus, it is extremely important to be aware of this situation and knowledgeable alternative procedures and tactics during surgery. This congenital defect is caused by an incomplete or malrotation of the intestine on the axis of the superior mesenteric artery during embryonic development.[3] About 90 percent of cases become clinically known in the first year after birth; however, some patients may remain asymptomatic throughout life.4 This paper aims to present the video-documented case report of patient with morbid obesity that successfully underwent laparoscopic single anastomosis gastric bypass (minigastric bypass) where this condition of intestinal malrotation was revealed at surgery. If the duodenojejunal angle is not correctly seen, as is generally the case, there is a risk of creating an antiperistaltic anastomosis.With careful measures, the procedure was completed laparoscopically, without any post-operative complications.When intestinal Malrotation is discovered unexpectedly in complex advanced laparoscopic procedures, it poses significant challenge.
Case report:
A 26-year old male patient with morbid obesity and a body mass index (BMI) of 50.4kg/m2 with no other comorbid conditions was scheduled for laparoscopic single anastomosis gastric bypass (SAGB, commonly called “mini” gastric bypass, after thorough preoperative assessment.
During surgery, a long, narrow gastric tube was created with gastric division from the lesser curvature, using a 36 French gastric calibration tube. We attempted to identify the ligament of Treitz in the left upper quadrant; however, we were surprised to find the terminal ileum and the appendix on the left side and entire small bowel on right side of the abdomen.
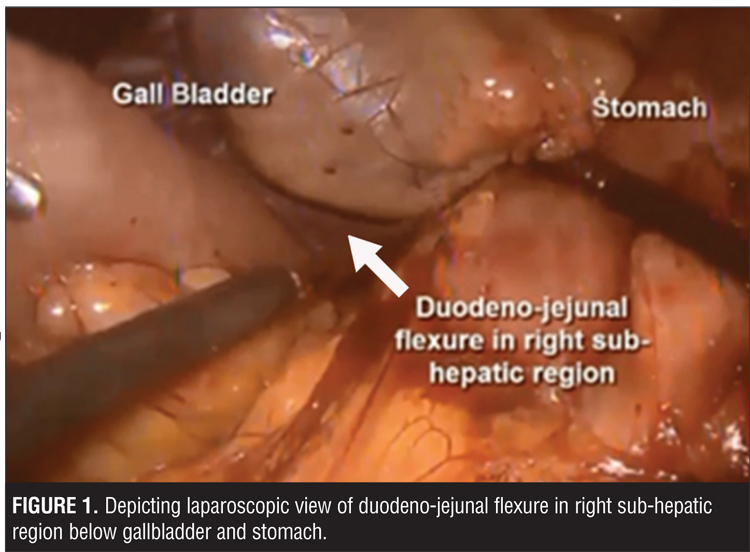
Intraoperatively, the duodenojejunal flexure was located in the right hypochondrium below the gallbladder (Figure 1) instead of conventional anatomical location on the left side, with entire small bowel loops on the right side. Thus, the diagnosis of intestinal malrotation was confirmed, and the jejunal loops were followed from the right sided duodenojejunal flexure for 210cm. Gastrojejunal anastomosis was performed.
This case emphasizes the importance of correctly identifying the ligament of Trietz and highlights the risk of inadvertent antiperistaltic anastomosis in a patient with intestinal malrotation .
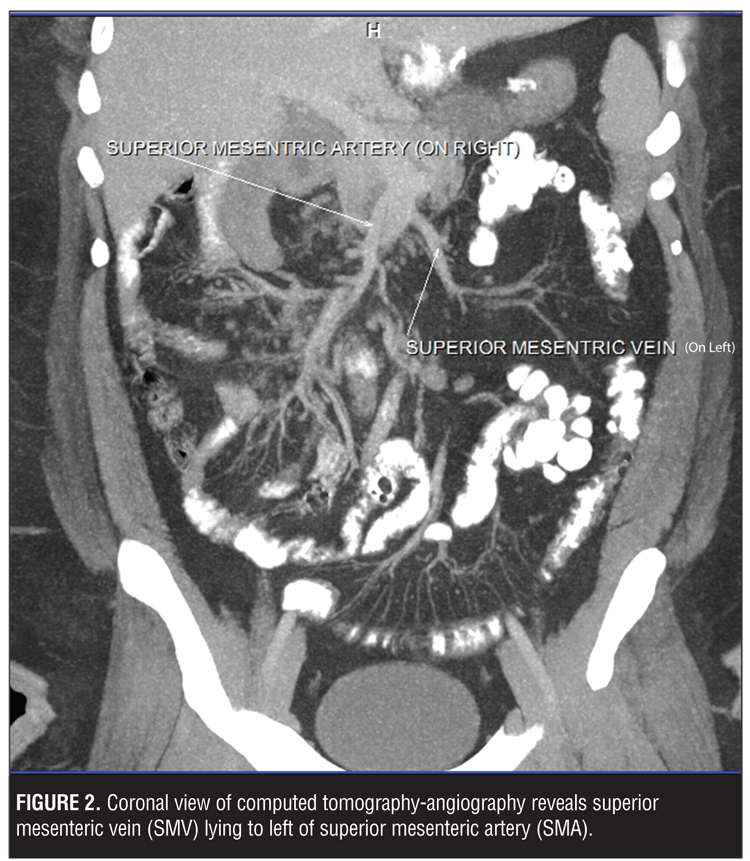
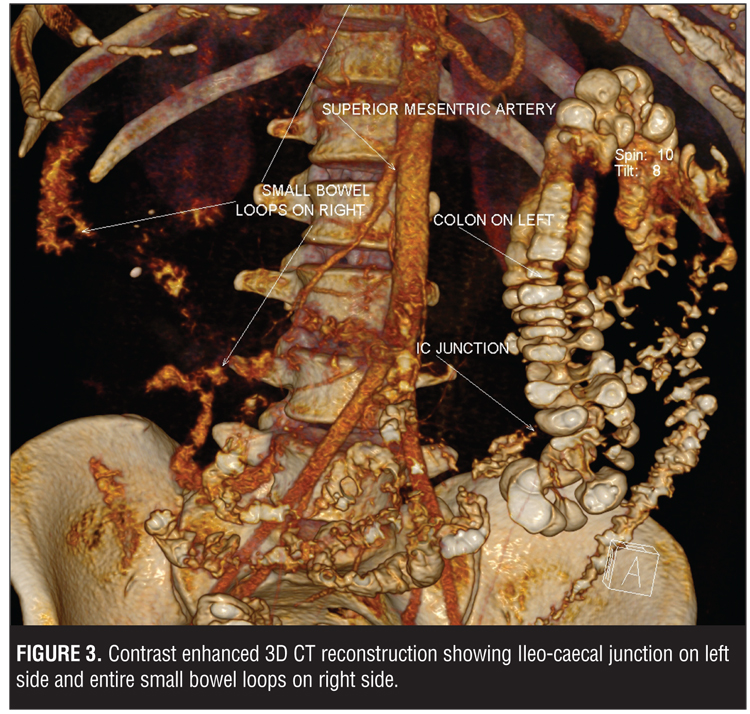
The patient had no postoperative complications, except for the expected weight loss, and is in regular clinical care follow up. Immediate postoperative gastrograffin study and computed tomography (CT) angiography (Figure 2) with contrast enhanced 3D CT reconstruction (Figure 3) showed superior mesenteric vein (SMV) lying to the left of superior mesenteric artery (SMA), confirming malrotation radiologically with levocardia.(Figure 4).
Situs inversus is frequently associated with dextrocardia; however, situs inversus with isolated levocardia, or simply isolated levocardia (ILC), is rare, with an incidence of 1 out of 22,000. and Situs inversus refers to a normal cardiac situs with the cardiac apex in the left hemithorax, in the presence of an aberrant arrangement of the abdominal organs.[14,15]
Discussion
Only a few descriptions of gastric bypass with intestinal malrotation are available in literature, and these are limited to clinical case reports.[1–9]
During embryonic development, the intestine undergoes three 90-degree counter-clockwise rotations around the axis formed by the superior mesenteric artery.[10]
These rotations occur simultaneously with the small bowel’s reintegration into the abdomen. After this, peritoneal fixation occurs between the end of the 12th week of development and birth. A malrotation describes rotation and fixation abnormalities with an abnormal relationship between the duodenojejunal angle and the ileocaecal valve, with abnormal colonic attachments. The complete common mesentery occurs when rotation stops at 90 degrees, the small bowel is located entirely on the right of the abdomen, the duodenojejunal angle is not clearly apparent and is located to the right of the mesenteric vessels, and the cecum is located in the left iliac fossa. The small bowel mesentery and colonic mesentery are, therefore, continuous in the same plane. Other rotation abnormalities, such as total absence of rotation, inverse rotations, and over-rotations are even more rare.
These rotation abnormalities may be suspected in adults as a result of ultrasound, upper gastrointestinal studies, or CT scans. These investigations are not routinely performed before bariatric surgery. In our case, an ultrasound to investigate for gallstones did not provide a preoperative diagnosis and X-ray of the chest showed levocardia (Figure 4). It is extremely difficult to investigate for the mesenteric vessels by ultrasound in patients with obesity, which is why the finding was not made preoperatively.
It is highly recommended that surgeons check that no abnormalities are present in the angle of the Treitz ligament before dividing the stomach. The anatomical abnormalities that should alert the surgeon include the following: a duodenojejunal angle on the right of the mesenteric vessels, absence of a transverse colon across the abdomen, the small intestine on the right side of the abdomen, and the cecum on the left. If uncertain, the whole small intestine should be traced in order to identify both ends. For this reason, the golden rule in performing a gastric bypass is to clearly visualize the duodenojejunal angle. This will allow an unknown bowel malrotation to be identified. Following this case, the study of the eso-gastro-jejunal transit as part of pre-operative assessment to screen for an abnormality of the angle of the esophagus and cardia as well as looking for malrotation may be suggested.
There are no video-documented descriptions of single anastomosis gastric bypass (minigastric bypass) with intestinal malrotation, and these are limited to clinical cases. To our knowledge, this is the first video-documented case of single anastomosis gastric bypass with intestinal malrotation with levocardia for morbid obesity. The golden rule in performing a gastric bypass is to clearly visualize the angle of the Treitz ligament which allows an unknown bowel malrotation to be identified. Bariatric surgeons need to be aware of the potential of such intraoperative surprises.
Acknowledgement
From Dr. Chintan B. Patel: My sincere thanks goes to Professor Dr. Ajay H. Bhandarwar who provided an opportunity for me to join his team and who conducted this surgery. Without his precious support, it would not have been possible to publish this report.
I would like to express my sincere gratitude to Dr. T.P. Lahane, Dean of the Grant Government Medical College & Sir J.J. Group of Hospitals in Mumbai, India, for supporting the Bariatric and Minimally Invasive Surgery Unit.
References
1. Alami RS, Schuster R, Morton JM, Curet MJ. Robotic-assisted laparoscopic Roux-en-Y gastric bypass in a patient with midgut malrotation. Surg Obes Relat Dis. 2002;2:222–22
2. Gagne DJ, Dovec EA, Urbant JE. Malrotation—an unexpected finding at laparoscopic Roux-en-Y gastric bypass: a video case report. Surg Obes Relat Dis. 2011;7:661–663.
3. Zissin R, Rathaus V, Oscadchy A, et al. Intestinal malrotation as an incidental finding on CT in adults. Abdom Imaging. 1999;24:550–555.
4. Alam I, Mahmud S, Ackroyd R, Baxter JN. Laparoscopic gastric bypass in a patient with malrotation of the intestine. Obes Surg. 2006;16:777–779.
5. Brauner E, Mahajna A, Assalia A. Intestinal malrotation presenting as midgut volvulus after massive weight loss following laparoscopic sleeve gastrectomy: case report and review of the literature. Surg Obes Relat Dis. 2012;8:e52–e55.
6. James AW, Zarnegar R, Aoki H, Campos GM. Laparoscopic gastric bypass with intestinal malrotation. Obes Surg. 2007;17:1119–1122.
7. Palepu RP, Harmon CM, Goldberg, SP, Clements RH. Intestinal malrotation discovered at the time of laparoscopic Roux-en-Y gastric bypass. J Gastrointest Surg. 2007;11:898–902.
8. Tayyem R, Sidkiqui T, Ali A. Midgut malrotation encountered during laparoscopic Roux-en-Y bypass. Obes Surg. 2009;19:1716–1718.
9. Gagne DJ, Dovec EA, Urbant JE. Malrotation-an unexpected finding at laparoscopic Roux-en-Y gastric bypass: a video case report. Surg Obes Relat Dis. 2011;7:661–663.
10. Helardot P, Bienayme J, Bargy FG. Chirurgie digestive de l’enfant. Doin, Paris; 1990: 369–382.
11. Kapfer SA Rappold JF. Intestinal malrotation-not just the pediatric surgeon’s problem. J Am Coll Surg. 2004;199:628–635.
12. Lointier P. Le Journal de Coeliochirurgie.
13. Brauner E, Mahajna A, Assalia A. Intestinal malrotation presenting as midgut volvulus after massive weight loss following laparoscopic sleeve gastrectomy: case report and review of the literature. Surg Obes Relat Dis. 2012;8:e52–e55.
14. Ghawi H, Zghouzi MM, Emahbes TM, Awad SM. Prenatal diagnosis of isolated levocardia and a structurally normal heart: two case reports and a review of the literature. Pediatr Cardiol. 2013;34(4):1034–1037.
15. Vijayakumar V, Brandt T. Prolonged survival with isolated levocardia and situs inversus. Cleve Clin J Med. 1991;58(3):243–247.
FUNDING: No funding was provided.
DISCLOSURES: The authors report no conflicts relevant to the content of this article.
Category: Case Report, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}