
The Hole in the Wall with Samuel Szomstein, MD, FACS
Dedicated to providing a venue for interactive exchange of ideas,
interesting topics, and surgical pearls from experts in repair of
abdominal wall defects as they relate to bariatric surgery
A Message from Column Editor
Samuel Szomstein, MD, FACS
Dr. Szomstein is the Associate Director of the Bariatric Institute and Section of Minimally Invasive Surgery at the Cleveland Clinic in Weston, Florida, and Clinical Associate Professor of Surgery, Florida International University
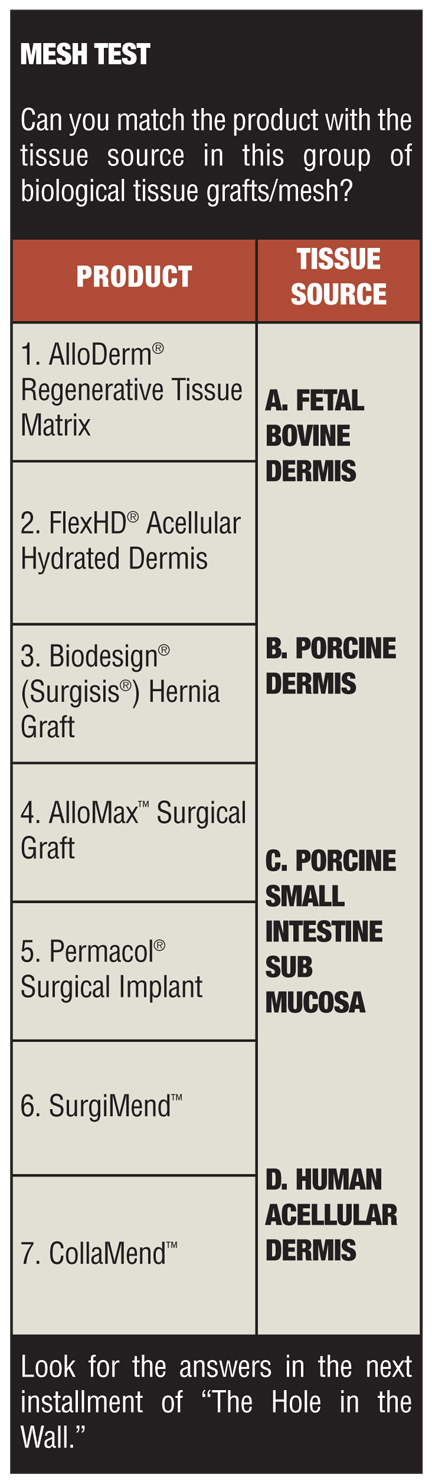
Welcome to the first installment of “The Hole in the Wall.” The purpose of this column is to provide the readers of Bariatric Times with a venue for an interactive exchange of ideas, interesting topics, and surgical pearls from experts in the field of abdominal wall defect repair as they relates to bariatric surgery. We encourage your questions, ideas, and surgical scenarios in what we are certain will be an interesting and educational column. We are very honored to have Martin I. Newman, MD, FACS, Head of Clinical Research, Plastic Surgery; Associate Program Director and Education Director, Cleveland Clinic Florida and Clinical Professor of Surgery, Florida International University, as our first guest expert. We welcome his expertise and comments in this month’s installment, “Abdominal Wall Reconstruction in the Massive Weight Loss Patient.” We also encourage you to take “the Mesh Test” at the end of this article and see how you do. We hope you enjoy our column, and we look forward to your questions, comments, and participation in future installments.
Abdominal Wall Reconstruction in the Massive Weight Loss Patient
by Martin I. Newman, MD, FACS
Dr. Newman is the Associate Program Director, Department of Plastic Surgery, Education Director, Weston, Diplomate American Board of Surgery, Diplomate American Board of Plastic Surgery, Cleveland Clinic Florida, Weston, Florida
Bariatric Times. 2011;8(4)16–17
Abdominal wall defects in the individuals who have undergone bariatric surgery and have experienced massive weight loss are unique in two respects. First, abdominal wall defects often develop in patients with exceedingly high body mass indices (BMIs) prior to bariatric surgery and prior to significant weight loss. Second, they occur in a patient population whose tissues have suffered the damage associated with massive weight gain followed by massive weight loss. Thus, the surgical approach to abdominal defects in this patient population must be specialized and tailored for the unique set of circumstances that surround their development as well as the global patient presentation in which repair is contemplated.
STRATIFICATION
Several stratification models exist for the classification of abdominal wall defects. Generally, they are based on the size of the defect, the presence or absence of infection, comorbid conditions, and/or a history of previous hernia. Although most of these stratification models are adequate, we have previously described a classification strategy for abdominal wall defects that works well in our practice—Grades I–IV.1 Although subjective in many ways, we find that Grades I–IV is a helpful method of assessment and surgical planning.
Grade I defects are small, less than 4cm, with no significant underlying medical conditions. These are, in our practice, repaired with traditional surgical techniques with or without mesh.
Grade II defects are larger, 4–8cm, and are usually associated with a mild loss of domain. However, patients with these defects present without significant underlying medical conditions. We repair Grade II defects with the component separation technique, as described under the Procedure section of this article.
Grade III defects are greater than 8cm with significant loss of domain and/or significant underlying medical problems. We consider patients with Grade III defects at higher risk for recurrence than the smaller, more straightforward Grades I and II defects. In these cases, we combine our component separation repair with reinforcement. In our practice, this is best accomplished with a mesh overlay, biologic or synthetic, depending upon the character and quality of the overlying skin and subcutaneous tissue.
Grade IV defects are the largest and are associated with conditions that make component separation impossible. Examples of Grade IV defects include patients with frozen abdomens or patients with multiple defects and/or fistulas associated with “blown-out” or “swiss-cheese” abdominal walls. We use a variety of approaches to manage defects in these cases, including a combination of biologic and synthetic mesh bridges with the knowledge that second procedures may sometimes be necessary.
ABDOMINAL WALL DEFECTS IN THE POSTBARIATRIC POPULATION
In our experience, abdominal wall defects in the massive weight loss patient usually fall into the Grade III or IV. Although many of our postbariatric patients have lost in excess of 100 pounds, many present to us with a BMI greater than 30kg/m[2]. This alone places them at high risk for recurrence. Also, the defects seen on presentation have usually developed years earlier, prior to bariatric surgery, and, therefore, initiated and “grew” when the BMI was much higher, in some cases approaching or exceeding 40kg/m2. As a result, the abdominal wall musculature is attenuated and the normal anatomy is distorted. The best approach, in our practice, is to repair these defects with a component separation followed by reinforcement with biologic or synthetic mesh. When primary closure following component separation is not possible, however, a bridge repair is the best option.
The choice of which mesh to use, biologic or synthetic, in our practice depends upon the presence or absence of infection and the character and quality of the overlying skin. In an infected or contaminated surgical field, we would never recommend placing a synthetic mesh. Also, if the character and quality of the overlying skin suggest a high risk of a wound breakdown, we avoid placing a synthetic mesh as an overlay. In contrast, an underlay mesh may be better protected in these special situations.
Although our technique for component separation is not unique, there are some steps in the procedure that deserve additional discussion. The following is an outline of the procedure as we perform it in the patient who has experienced massive weight loss with special attention given to the factors mentioned previously.
THE PROCEDURE
In our practice, we employ a multidisciplinary approach to abdominal wall defects. Our general surgical colleagues begin by opening the wound, reducing the hernia, and performing lysis of adhesions. Preservation of the hernia sac is dependent upon the defect and the nature of this structure. We help design the opening incision and usually request that it extend from xiphoid process to pubis, even if the defect is isolated to the epigastric or infraumbilical midline. A full midline incision is helpful because it allows tension to be distributed along the maximum length of the wound which, in our opinion, helps to reduce tension at any particular point along the length of the wound.
Once the hernia is reduced and the lysis of adhesions has been completed, we begin raising skin flaps. A skin flap is raised from the midline wound toward the anterior axillary line on the right and then on the left. During this portion of the procedure, we leave a cuff of subcutaneous fat adherent to the abdominal wall fascia because it is theorized that this will reduce the risk of seroma. The evidence for this is anecdotal, but in our practice, it seems to reduce seroma formation. The need to dissect the skin flaps as wide as the anterior axillary line has been questioned. We argue that a full dissection is beneficial because it helps to reduce tension on the midline. Undermining is a well-established plastic surgical principal, and we find it helpful in these cases.
Following exposure of the anterior abdominal wall musculature, we then identify the lateral border of the rectus sheath. Our first relaxing incision is made approximately 1cm lateral to the lateral border of the rectus sheath. This is in ideal location because it represents the tendinous insertion of the external oblique muscle into the rectus sheath. This is a bloodless plane, and division of this tendinous portion of the external oblique can be accomplished quickly and effectively with cautery, cold knife, or surgical dissection scissors. In our practice, we use cautery with care to establish hemostasis of intercostal perforating vessels, which may become apparent. The lateral portion of the external oblique muscle is then lifted (e.g., separated) from the underlying internal oblique muscle. This can be achieved with minimal dissection through the embryologic areolar plane. We perform the dissection with cautery but note that it might also be easily accomplished using blunt dissection. This “separation” maneuver can provide up to 10cm of excursion in some patients, but most often provides between 6 and 8cm of advancement. In patients who have had large defects for long periods of time (i.e., greater than one year), we find that the excursion falls toward the lower end of these numbers. In patients who have defects that are not as long-standing (i.e., less than one year), excursion is usually greater.
Should the separation of the external oblique muscle at the tendinous portion not provide us with enough excursion to achieve a tension-free closure along the midline, a second relaxing incision is made on the posterior aspect of the rectus sheath. This incision is made with cautery slowly to ensure hemostasis, and is carried out along the longitudinal access of this type III muscle. The team is careful to avoid violation of either the superior or inferior pedicle found on the posterior aspect of the rectus abdominous, for doing so would result in blood loss. As a type III muscle, complete ligation of either the superior or inferior pedicle can occur without ischemic damage to the muscle. However, it is not necessary to ligate these vessels, and preservation may be well appreciated should the rectus muscle be required to reconstruct an unanticipated defect sometime in the future (transverse rectus abdominis myocutaneous [TRAM], vertical rectus abdominis myocutaneous [VRAM]).
Once the relaxing incisions have been made, the right and left rectus muscles can be advanced toward the midline as bilateral, bipedicle advancement flaps. If this can be achieved in a tension-free manner, the abdominal wall is closed primarily. In our practice, we use a number one looped polydioxanone (PDS) suture. One suture is run from the inferior and one from the superior, which then meet and are tied in the middle.
Reinforcement is then performed with a biologic or synthetic mesh. In our practice, we find that it is important to incorporate the most lateral portions of the external oblique in this closure. In other words, the mesh is sewn to the medial margin of the most lateral tendinous portion of the right external oblique muscle, drawn over the midline, and secured to the analogous structure on the contralateral side. When necessary, this maneuver is performed as an underlay prior to closure of the midline defect. In the same fashion, it is important to capture the medial margin of the lateral external oblique in the closure for it provides, in our opinion, the best reinforcement.
The next step involves closure of the skin. Drains are critical and in our practice we use two number 19 large, round drains to completely cover the anterior abdominal wall and the repair area. They are brought out along the right and left lower quadrant, respectively, and are secured with a 0 silk suture in anticipation for a long drain course. It is not uncommon for these drains to remain in situ for 3 to 4 weeks. During the placement of the drains, the team is careful to not place them directly through the skin in a perpendicular fashion, but rather to run them in the subcutaneous space for 3 to 4cm to encourage a cuff of subcutaneous tissue separating the potential space from the skin.
Closure of the skin should be detailed as well. A layered closure is a well-established plastic surgical principal, and rather than simply stapling the skin closed, Scarpa’s fascia is closed with 2-0 PDS suture in interrupted fashion. Finally, the skin is closed with staples or 4-0 subcuticular absorbable suture depending upon the case and the surgeon’s preference. If staples are used, we coat the wound with a bacitracin ointment and cover this with xeroform dressing, which is left in place for three days. If absorbable sutures were used, a skin sealing is used as the final dressing.
POSTOPERATIVE MANAGEMENT
Some postoperative points deserve mention. For example, in our practice, a nasogastric tube is placed intraoperatively and left in place until the patient demonstrates flatus in the postoperative period. This may reduce the risk of ileus, which itself may compromise the repair if excessive. An anticoagulant may be used at the surgeon’s discretion according to protocol, but care should be taken not to inject heparin or enoxaparin sodium into the abdominal flap. Although evidence for this is anecdotal, we do theorize that subcutaneous administration of an anticoagulant medication into the abdominal flap may increase the risk for subcutaneous hematoma. We allow our patients to shower with the drains. Early ambulation is advised. Long-term restrictions are placed on these patients, and our protocol is that abdominal wall reconstruction should be followed by at least two weeks of rest followed by one month of light duty. However, we encourage patients not to place a stress upon the abdomen (e.g., abdominal exercise, heavy lifting) for up to six months following abdominal wall reconstruction.
Our patients are followed in clinic, every 7 to 10 days on average until the drains come out. After this, a return visit for “seroma check” may be helpful for some patients. Should a seroma be identified, management should be at the discretion of the operating surgeon. In our practice, we are aggressive with seromas and prefer drainage in most cases.
CONCLUSION
In summary, abdominal wall defects in the massive weight loss patient present unique challenges. These patients can often be helped with the component separation operation with attention to some of the principal outlined in this column.
References
1. Newman MI. Reducing the incidence of recurrence in component separation repair. General Surgery News. 2009;9:36.
Category: Hole in the Wall, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}