
Weight Loss before Weight Loss Surgery: What Do We Know About Dropping Those Preoperative Pounds?
by Liz Goldenberg, MPH, RD, CDN
Ms. Goldenberg is from New-York Presbyterian Hospital, Weill Cornell College of Medicine of Cornell University, Department of Surgery, New York, New York.
Bariatric Times. 2010;7(7):18–20
Abstract
This article reviews the issues surrounding weight loss before surgical weight loss, and aims to answer the questions that weight loss surgery centers might have when making decisions about including a preoperative weight loss component in their surgical programs.
Introduction
Weight loss surgery is growing in popularity. According to the American Society for Metabolic and Bariatric Surgery (ASMBS), there were 220,000 bariatric surgeries performed in 2008 and this number is on the rise. Considering that approximately five percent of American adults meet the criteria for morbid obesity, a large pool of surgical candidates remain.[1] As more operations are being performed and the morbidity and mortality statistics of these surgeries remain favorable, older and sicker patients may be finding their way to the bariatric surgeon’s office. These patients are considered to be at higher risk for complications, since age and the presence of medical comorbidities, along with male gender, body mass index (BMI), and fat distribution, have been identified among the factors that negatively impact the safety of the operation. Of these factors, few can be altered except BMI and fat distribution.
Physicians can choose to operate on higher risk patients by modifying the procedure, perhaps by performing a sleeve instead of, or prior to, a Roux-en-Y gastric bypass (RYGB).
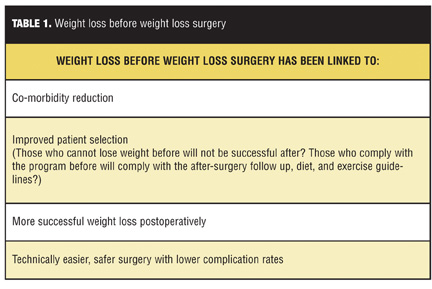
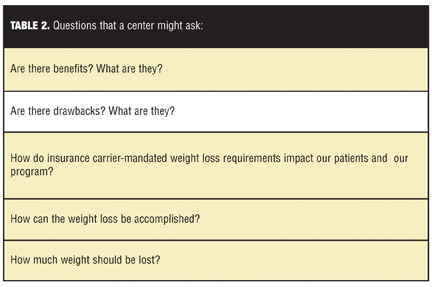
Another option for bariatric programs to deal with higher risk candidates is by recommending, or in some cases mandating, weight loss prior to undergoing weight loss surgery. Some surgery centers recommend preoperative weight reduction for all of their patients, for the reasons listed in Table 1. Table 2
Benefits to Preoperative Weight Loss
The liver, operative time, and length of stay. A number of studies have found benefits to preoperative weight loss. Liu et al[2] compared patients who did and who did not lose weight before surgery and found that those who lost weight were more likely to undergo surgery that did not deviate from the standard RYGB operation. Additionally, patients who did not lose weight were more likely to have their surgeon comment that the patients’ livers were enlarged. The authors did not find differences in operative time, length of stay, major complications, or wound infections between the groups.
There are a number of studies that look at the effects of weight loss on the liver. Benjaminov et al[3] found a reduction in liver volume of 8.1 percent, as well as a nonobjective observation by surgeons that this facilitated surgery, in patients who lost weight in the four weeks prior to surgery. In the six weeks prior to surgery, Lewis et al[4] accomplished an even greater reduction in mean liver volume of 14.7 percent, as well as a 43-percent decrease in mean liver fat. Both a reduction in liver size and operative time was achieved in a small group of patients who lost an average of 4.8kgs, also in a six-week time frame prior to surgery.[5] Operative times were found to be a highly significant 36 minutes shorter in 62 out of 90 patients who were able to lose more than five percent of their preoperative weight.[6] Still et al[1] calculated that length of stay was less likely to be greater than four days in high-risk patients who were able to lose 5 to 10 percent of their excess weight before undergoing RYGB. It has been pointed out that high-risk patients may experience a greater benefit from preoperative weight loss.[15]
Overall complications. The overall major complication and mortality rates of bariatric surgery are quite low, less than 3.0 percent and 0.3 percent, respectively. Studies have shown mixed results as to whether preoperative weight loss lessens postoperative complications. Not only have some studies been unable to find fewer complications for those that lost,[6,7] but in one study[8] even preoperative weight gain did not negatively impact complication rates.
However, considering the low overall complication rates of bariatric surgery, among the criticisms of these studies are that they involved inadequate sample sizes of 200 patients or less. Benotti et al[9] reviewed the records of 881 RYGB patients for categories of complications including the following: respiratory issues, bleeding, gastrointestinal issues, feeding intolerance, cardiac issues, leakage, infection, thromboembolism, acute renal failure, urinary issues, wound issues, and stricture. The reviewers found statistically significant trends that confirmed a diminishing likelihood of any complication with increasing preoperative weight loss.
Impact on postoperative weight loss. There has been some conflicting data as to whether successful weight loss preoperatively will translate into more successful postoperative weight loss. In 2005, Alvarado et al[6] reported that preoperative weight loss was associated with greater weight loss at one year postoperatively, specifically an increase of one percent of preoperative weight loss for a 1.8-percent increase after surgery. This occurred despite the fact that 83 percent of the patients in the study failed to achieve the recommended 10-percent weight loss. In 2008, Alger-Mayer et al[10] described a more successful weight loss achievement, as well as a significant correlation between weight lost before and at three years after surgery. One-hundred and fifty patients who were advised to lose 10 percent of their initial presenting weight were able to realize a 9.5±6.8-percent loss before undergoing gastric bypass. The authors attribute their positive results to the implementation of physical activity and positive dietary changes early, and they point out that their patients credit their success to the same factors. Another possible explanation is that those patients who were able to achieve greater weight loss before surgery are the same patients who are more likely to follow up and adhere to the guidelines afterwards. A review article by Livhits et al[11] compiled data from 15 different papers comparing weight loss before and after surgery. This large synopsis came to the same conclusion that preoperative weight loss results in greater total postoperative weight loss.
Contrary to the collection of studies mentioned previously are papers by Jantz et al[12] and Ochner et al.[13] In 2009, Jantz et al[12] failed to find a correlation between the percentage of excess weight loss (EWL) at one year postoperatively and the maximum amount of weight loss achieved prior to surgery. However, this was looking at self-reported weight loss and did not necessarily occur in the short period of time prior to surgery. In an even more recent paper published in Obesity in February 2010, Ochner et al[13] found that more weight gain was predictive of more weight loss after surgery. This study only looked at the three-month postoperative visit and, perhaps more importantly, compared patients who were mandated to undergo a six-month, physician-supervised weight loss program prior to surgery to those who did have this requirement. On average, more than 75 percent of patients in both groups gained weight before surgery. Surprisingly, at three months postoperatively, these same “gainers” had lost more weight than those who has lost weight prior to their operation. Authors propose that diet fatigue or the “last supper syndrome,” which occurs when patients intentionally over-eat, or binge on their favorite foods for fear that they will miss this habit or these foods after surgery, may be responsible. This binge-eating behavior is squelched postoperatively by the new, tiny pouch. Finally, the authors point out that the biological set-point theory may play a role in why patients who lose more weight prior to surgery lose less after.
Drawbacks to Preoperative Weight Loss or Preoperative Weight Loss Programs
While there is some trepidation over the safety of encouraging rapid weight loss in patients who are months or weeks away from major surgery, this author is unaware of any negative clinical outcome reports. Nevertheless, there are a handful of drawbacks to consider by a surgery center looking to implement this type of program. One downside is the cost to the program in staffing and other resources. The programs are usually administered by registered dietitians, physicians who are part of a medical weight loss arm of the program, or, in some programs, surgeons or gastroenterologists who may place a device, such as an intragastric balloon. While programs usually include an exercise component to them, few studies mention the utilization of a trained exercise specialist.
Another possible deterrent may be the concern of patients dropping out of the program. A well-designed preoperative weight loss program may go on for as little as two weeks or as long as six months, which is a significant delay. Programs may argue that delaying surgery may deter patients from ultimately having the surgery. Alami et al[7] discuss this fear but did not find a delay; the times from consultation to operation (approximately five months) were similar in the groups that did and did not undergo a preoperative weight loss program. One patient in this study left to have surgery at a center that did not have this requirement.
Weight loss attempts required by insurance carriers versus the surgeon. Insurance-mandated preoperative weight loss programs have become a routine delay. Preoperative weight loss interventions are assumed to improve outcomes by increasing weight loss and subsequently the positive aspects of weight reduction. Many feel that these programs are meant to be a test of patients’ motivation.
Two studies aimed to challenge the merit of this prerequisite by comparing sets of patients who were required to undergo an insurance-mandated preoperative program with those who did not have this requirement. Researchers in one study reported that 28 percent of patients commanded to follow the registered dietitan-supervised 13-week program dropped out of the program, as compared to only 19 percent of the group free from this requirement.[14] Both groups were more likely to gain versus lose weight prior to surgery. Both groups had similar total weight loss at one year, yet the patients who did not have the mandated delay achieved a greater percentage of EWL that was significant at the one-year mark. The recent study in Obesity by Olchner et al[13] came to a similar conclusion when comparing groups of patients with or without insurance requirements.[13] The 94 patients who had to fulfill the requirement gained weight preoperatively; an average of 2.9±4.4 percent of their initial body weight.
Olchner et al propose that some patients fear that successful weight loss may lead to insurance denial for the surgery. Both studies accused insurance-required programs of being obstacles to patient access to surgical treatment of obesity, in addition to not being effective at bringing about preoperative weight loss.
In contrast to the studies by Olchner et al[13] and Jamal et al,[14] the 150 patients in the study by Alger-Mayer et al[10] were required by their surgeon and not by their insurance carrier to undergo a diet and exercise program. All patients that wished to undergo surgery at this practice, regardless of presenting BMI, were expected to follow the program and lose 10 percent of their initial documented weight. Instead of a 28-percent drop out rate, reportedly only one of their patients left to go to another practice that did not require preoperative weight loss.
Preoperative Weight Loss Methods
Many patients with obesity seeking weight loss surgery are actually quite adept at losing weight. They are able to take off the weight for a short period, usually through diet and/or exercise, but then find themselves rebounding, gaining back part, all, or even more weight than they initially lost. Others find that the difficulty occurs when they reach that plateau of 10, 20, or 50 pounds and the scale is at a stand-still. On the other hand, some patients have never in their lives successfully lost weight. Regardless of the history, patients who appear in the surgeon’s office can become a highly motivated bunch if told by the surgeon that they will not be operated on unless they lose weight beforehand. As described previously, aside from or in addition to surgeons making these demands on patients, many insurance providers place demands on doctors to supervise their patients’ weight loss efforts in order for them to get coverage. However, most health insurance plans do not specify any particular type of program for providers to follow. As surgical programs looking to accomplish preoperative weight loss, what are the options?
Diets, Medication, and a Device. Dieting is the method of weight loss most often cited in studies that look at weight loss prior to surgery. This could be because most weight loss surgery programs already have dietitians either as part of their team or as consultants who carry out preoperative evaluations (as required to fulfill National Institutes of Health [(NIH)] criteria, by insurance companies, and for ASMBS Centers of Excellence [(COE)] or American College of Surgeons [(ACS)] Bariatric Surgery Center Network [(BSCN)] certification). As pointed out previously, few programs have exercise experts on their teams, probably because they are not required by the above organizations. Yet plenty of evidence backs the synergism of diet plus exercise, or the effects of an entire multidisciplinary team including these providers previously noted along with psychologists or behavioral therapists, in bringing about weight loss.
The diets that have reportedly been used for bringing about preoperative weight loss range from a vague “healthy balanced diet,” to a strict very low-calorie, liquid diet,[2,4] to a very low carbohydrate (30g) diet,[3] to a highly involved and resource-consuming, supervised 11-week inpatient weight loss program.[15]
Which type of diet is the most effective is the topic of another paper, but there are two common denominators to be found among the conclusions to studies that compare the efficacy of various weight loss diets. The first is that those who stay on the diet lose the most weight, and the second is that patients who have a say in which diet they follow (versus having to follow a diet that is chosen for them) will be more successful.[16,17] One can see how these two suggestions are interdependent. A final point on choice of diet is that although these may seem to be common-sense recommendations, they can be easily overlooked by programs that routinely use standard diet plans and thus fail to individualize plans according to patients’ preferences.
One study[5] looked at the effectiveness of sibutramine (Abbott Laboratories, North Chicago, Illinois) in preoperative weight loss. Twenty patients received 15mg of this medication once daily for six weeks, while another 20 patients did not. The medication group lost 4.8kg while the control group gained 7.0kg and spent an additional 20 minutes in the operating room when compared to the patients who took sibutramine.
There are two reports on the use of an intragastric balloon for preoperative weight loss.[18,19] Thirty-one and 75 patients achieved 22 and 16-percent EWL, respectively, after the device was implanted for at least six months. There was no operative mortality and only two patients in each of the studies suffered from intolerance and had to have the balloon removed soon after implantation.
How Much Weight Should Be Lost?
There is a scarcity of data comparing the pros and cons of how much weight should be lost. Though insurance companies often mandate that the attempt must be made, they rarely make specific recommendations as to the amount of weight loss.[13] This is likely because it is difficult to draw conclusions from existing data. One reason for the difficulty is that a standard definition for how to report weight loss is lacking. Some studies report on total weight loss or percentage of total weight loss, while others use EWL or percentage of EWL, and still others use excess BMI loss. Another issue is a lack of prospective, randomized trials; most papers are retrospective reviews.[20]
Many papers support 5- to 10-percent total weight loss or the same amount of excess weight loss as a desirable goals.[1,7,11] Evidence for this goal is seemingly derived from studies that link this range of weight loss to significant reductions in obesity-related comorbidities. Most would agree that more quality data are needed in order to draw evidence-based conclusions on the ideal amount of weight loss that should be recommended.
Even if studies were forthcoming, realistic versus optimistic weight loss is an important distinction in this group. Patients who are typically 100 or more pounds away from their ideal body weight and have a history of “failed” dieting attempts will continue to be challenged by the irony of trying to lose weight before undergoing an operation that will give them help to achieve the same result.
Conclusion
In summary, whether programs should suggest or require weight loss before weight loss surgery and whether it should be for all patients or only for select groups, such as high-risk patients, will probably continue to be a controversial decision to make. Barring any mandates from insurance carriers or accreditation programs, surgery centers will likely continue to decide for themselves whether it is in theirs, and of course their patients’ best interests to promote the dropping of those preoperative pounds.
References
1. Still CD, Benotti P, Wood GC, et al. Outcomes of preoperative weight loss in high-risk patients undergoing gastric bypass surgery. Arch Surg. 2007;142(10):994–998.
2. Liu RC, Sabnis AA, Forsyth C, Chand B. The effects of acute preoperative weight loss on laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2005;15(10):1396–1402.
3. Benjaminov O, Beglaibter N, Gindy L, et al. The effect of a low-carbohydrate diet on the nonalcoholic fatty liver in morbidly obese patients before bariatric surgery. Surg Endosc. 2007;21(8):1423–427.
4. Lewis MC, Phillips ML, Slavotinek JP, et al. Change in liver size and fat content after treatment with Optifast very low calorie diet. Obes Surg. 2006;16(6):697–701.
5. Aberle J, Freier A, Busch P, et al. Treatment with sibutramine prior to Roux-en-Y gastric bypass leads to an improvement of metabolic parameters and to a reduction of liver size and operative time. Obes Surg. 2009;19(11):1504–1507.
6. Alvarado R, Alami RS, Hsu G, et al. The impact of preoperative weight loss in patients undergoing laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2005;15(9):1282–1286.
7. Alami RS, Morton JM, Schuster R, et al. Is there a benefit to preoperative weight loss in gastric bypass patients? A prospective randomized trial. Surg Obes Relat Dis. 2007;3(2):141–145; discussion 145–146.
8. Harnisch MC, Portenier DD, Pryor AD, et al. Preoperative weight gain does not predict failure of weight loss or co-morbidity resolution of laparoscopic Roux-en-Y gastric bypass for morbid obesity. Surg Obes Relat Dis. 2008;4(3):445–450.
9. Benotti PN, Still CD, Wood GC, et al. Preoperative weight loss before bariatric surgery. Arch Surg. 2009;144(12):1150–1155.
10. Alger-Mayer S, Polimeni JM, Malone M. Preoperative weight loss as a predictor of long-term success following Roux-en-Y gastric bypass. Obes Surg. 2008;18(7):772–775.
11. Livhits M, Mercado C, Yermilov I, et al. Does weight loss immediately before bariatric surgery improve outcomes: a systematic review. Surg Obes Relat Dis. 2009;5(6):713–721.
12. Jantz EJ, Larson CJ, Mathiason MA, et al. Number of weight loss attempts and maximum weight loss before Roux-en-Y laparoscopic gastric bypass surgery are not predictive of postoperative weight loss. Surg Obes Relat Dis. 2009;5(2):208–211.
13. Ochner CN, Puma LM, Raevuori A, et al. Effectiveness of a prebariatric surgery insurance required weight loss regimen and relation to postsurgical weight loss. Obesity (Silver Spring). 2010;18(2):287–292.
14. Jamal MK, DeMaria EJ, Johnson JM, et al. Insurance-mandated preoperative dietary counseling does not improve outcome and increases dropout rates in patients considering gastric bypass surgery for morbid obesity. Surg Obes Relat Dis. 2006;2(2):122–127.
15. Huerta S, Li Z, Anthony T, Livingston EH. Feasibility of a supervised inpatient low-calorie diet program for massive weight loss prior to RYGB in superobese patients. Obes Surg. 2010;20(2):173–180.
16. Brehm BJ, D’Alessio DA. Weight loss and metabolic benefits with diets of varying fat and carbohydrate content: separating the wheat from the chaff. Nat Clin Pract Endocrinol Metab. 2008;4(3):140–146.
17. Dansinger ML, Gleason JA, Griffith JL, et al. Comparison of the Atkins, Ornish, Weight Watchers, and Zone diets for weight loss and heart disease risk reduction: a randomized trial. JAMA. 2005;293(1):43–53.
18. Frutos MD, Morales MD, Luján J, et al. Intragastric balloon reduces liver volume in super-obese patients, facilitating subsequent laparoscopic gastric bypass. Obes Surg. 2007;17(2):150–154.
19. Mills S, Bassona S, Cornisha J, et al. Intragastric balloon use to reduce weight before bariatric surgery. Surg Obes Relat Dis. 2010;6(2):224.
20. Tarnoff M, Kaplan LM, Shikora S. An evidenced-based assessment of preoperative weight loss in bariatric surgery. Obes Surg. 2008;18(9):1059–1061.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}