Following Through: The Role of Intention in Physical Activity Adherence with Post-bariatric Surgery Recommendations
by Robin M. Stoops, MA, MS, CPT, and Cynthia L. Alexander, PsyD
Ms. Stoops and Dr. Alexander are from Cleveland Clinic Florida, Weston, Florida.
Financial disclosure: Ms. Stoops and Dr. Alexander report no conflicts of interest relevant to the content of this article.
Bariatric Times. 2011;8(3):18–19
Abstract
Participation in physical activity is recommended as part of a comprehensive plan for the bariatric patient. Many individuals struggle with consistent and long-term implementation of this component, despite intentions to engage in exercise. In this article, the theory of planned behavior is examined with regard to increasing bariatric patient’s exercise adherence, both pre- and postsurgery. The specific value of understanding perceived behavioral control in this process is also explored. Suggestions for program design based on these variables are offered.
Introduction
Physical activity (PA) recommendations have consistently been included as an integral component to a comprehensive weight loss and maintenance program for the bariatric patient.[1,2] Participation in a consistent PA program has been associated with numerous health-related benefits, including increased energy expenditure; decreased obesity-related complications, such as hypertension, hyperlipidemia, and type 2 diabetes mellitus; increased cardiorespiratory fitness; decreased cardiovascular disease risk; and mental health benefits, such as decreased anxiety, depression, and life stress.[3,4] In addition, patients who implemented a consistent PA program prior to bariatric surgery were found to exhibit increased rates of exercise participation and overall quality of life compared to those who did not engage in pre-surgical exercise.[5] Furthermore, engaging in PA post-surgery has been associated with weight loss of more than four percent of body mass index (BMI) as well as overall higher achievement rates of post-surgical goals compared to patients who did not incorporate exercise following surgery.[1,6]
Nonadherence to Exercise Recommendations
Despite these positive findings, nonadherence with behavioral recommendations, including physical activity and dietary suggestions, is pervasive following bariatric surgery. Although long-term rates are not yet known, one study found 40 percent of bariatric patients were not following through with physical activity at six months post-surgery, and 41 percent were not exercising at 12 months post-surgery.[7] A further study found only one-third of bariatric surgery patients engaged in the recommended amount of PA to prevent weight regain over a one-year period post surgery.[8] Specifically, PA has been found to be more difficult to enforce than nutritional recommendations, and one study found it to be the most likely area of nonadherence in a population of post-surgery bariatric patients.[1,7] It has also been suggested that patients lose weight post-surgery even in the absence of physical activity for a period of time, particularly over the first year, which may affect rates of implementation and adherence to PA in the short- and long-term.[3,7] Other commonly cited barriers to PA include perceived lack of time, self awareness while exercising in public environments; frustration with implementing PA recommendations into a consistent routine; comorbid conditions, such as musculoskeletal issues affecting mobility; and financial and transportation restrictions.[9,10]
Increasing Exercise Adherence
Given these concerns, it is beneficial to explore conditions that may influence and contribute to a greater likelihood of PA implementation and adherence to promote long-term change and improved quality of life for bariatric patients. Specifically, the construct of intention has been studied with regard to numerous health-related behavioral changes, such as exercise, smoking cessation, and alcohol use.[11] Intention encompasses motivational factors that influence behavior, which is described as the extent to which an individual is willing to try to perform the behavior.[11] With regard to PA, the intent to engage in exercise is the first step in a decisional path toward actually engaging in exercise behavior.[12] Intentions may change over time, particularly due to unanticipated events.[12] This may be particularly relevant with PA, where intentions could be thwarted by numerous perceived obstacles, such as weather, time, and finances.[4]
The role of intention in behavioral change has been examined through two social cognitive models, the theory of reasoned action (TRA) and the theory of planned behavior (TPB).[11–13] These models suggest examination of the intention to perform a behavior is the best predictor of behavior.[12] TRA addresses those behaviors that are volitional and suggests intention is a function of both the individual’s attitude toward the behavior (i.e., positive or negative evaluation of engaging in the behavior) and the subjective norm (i.e., the individual’s perception of social pressure to perform or not perform the behavior).[4,13] TPB expands on the concepts of TRA by including a third factor, perceived behavioral control (PBC). This refers to an individual’s perception of the ease or difficulty with performing the behavior. PBC consists of both internal (e.g., skills, emotions, information, self efficacy) and external (e.g., opportunities, dependence on others, constraints) factors.14 Individuals with morbid obesity may have lower levels of PBC, although initial rapid weight loss may increase PBC temporarily.[11] TPB also considers behaviors that are not entirely under volitional control in its model. PA among individuals with morbid obesity is not considered fully volitional due to additional weight and comorbid medical conditions, which can interfere with physical activity implementation and adherence.[11] In summary, the TPB model generally assumes individuals will have higher intentions of engaging in a behavior if they evaluate it positively, believe significant others approve of the behavior, and perceive they could easily perform the behavior.[11,14]
TPB’s relationship to PA has received noteworthy attention in the literature and has been found to be a superior predictor with exercise intentions and behavior compared to the TRA model.[4,11] An individual’s perception of control in a behavioral condition can greatly impact his or her motivation to perform the behavior.[12] Furthermore, an individual’s intention to try to perform the desired behavior is stronger when achievement of the goal is largely viewed as being under one’s own control.[12] However, research suggests PBC can lead to an accurate prediction of behavior only if the appraisal of the control is realistic.[4] This may be more likely in circumstances where an individual has prior experience with the behavior, in that a history of higher frequency of engaging in the behavior may correspond to a higher predictive value of engaging in the behavior in the future.4 In accordance with this hypothesis, those with moderate-to-high historical experience with PA may have more accurate perceptions of control related to the behavior compared to individuals with a low frequency of PA, thus increasing the predictive value of PBC.[4]
Findings from one study showed that bariatric patients’ intentions to engage in regular moderate PA increased the closer they were to their surgery date.[5] At this point, the patient may be more receptive to embracing the fundamental cognitive and emotional shifts away from their previous interfering behavioral patterns, which is necessary to sustain long-term change. The presurgical period may, therefore, be an ideal time to intervene to propose to the patient the possibility of a “new life” upon assuming responsibility for his or her own health.[1,15]
Targeting perceived behavioral control is another possible means of achieving increasing successful PA outcomes with post-surgery bariatric patients. Several studies found this factor to be the most significant of the TPB variables in terms of predicting PA intentions and self-reported participation in the behavior.[4,11,16] For example, Shifter and Ajzen[16] found participants who held strong intentions to lose weight combined with a high belief they could control achievement of this goal were more likely to lose weight than those with low levels of PBC. In terms of application, programs may experience higher rates of long-term success by focusing more on increasing PBC rather than providing education about exercise in an effort to change existing beliefs.[11] This is related to the assumption it is often easier to introduce information that may lead to the development of new beliefs rather than attempt to change current attitudes.[17 For example, targeted behaviors, such as increasing confidence, boosting sense of control toward PA, and encouraging PA in relationship to maintenance of weight loss, are all potential areas to address.[11] As previously stated, it is relevant to ensure the information provided leads to creation of realistic beliefs about behavioral control in order to impact long-term behavioral change.[4,17]
Development of a specific plan is also contributory to PBC and following through with PA intentions.[4,17 This consists of an individualized plan that considers how to incorporate PA into daily life, as well as what to do when difficulties or obstacles are encountered.[16] This has also been referred to as an implementation intention and includes the how, when, and where of following though with an intention.[18] The setting of mini goals has also been recommended to increase PBC by encouraging familiarity and increasing success with the intended behavior.[4] An environmental intervention may also be included as a component of the overall plan, which can boost PBC through increasing resources and opportunities, such as an employer-supported 30-minute walking program incorporated into the workday.[4,11]
When discussing PA, patients often look to professionals for recommendations, particularly if individuals have unsuccessful or negative experiences associated with the intended behavior (i.e., low PBC). This can also serve as an opportunity to enhance PBC by increasing an individual’s belief that he or she will be able to control achievement of the behavioral goal, as well as to reinforce realistic attempts. The use of an exercise specialist as a member of the bariatric team is suggested to be useful for this purpose, preferably in conjunction with previously discussed efforts to specifically increase PBC.[2,11,19]
Physical Activity Recommendations
Currently, there are no PA guidelines specifically for bariatric patients.[1,6] The most widely used recommendation is taken from the American College of Sports Medicine (ACSM), who suggest adults with overweight work toward 150 minutes weekly of moderate or higher-intensity PA.[20] Patients should be encouraged to move toward meeting or exceeding this recommendation until specific guidelines have been developed for bariatric patients.[21] The American Society for Metabolic and Bariatric Surgery (ASMBS) further recommends patients begin mild exercise (i.e., 20 minutes daily, 3–4 times weekly) pre-surgery, with walking also encouraged on Postoperative Day 1.[6] Walking is endorsed as the easiest and safest way for many bariatric patients to establish regular PA both pre and post-surgery, and the additional use of a pedometer has been found to be useful in goal setting and maintenance of PA over the long term.[1,6,19]
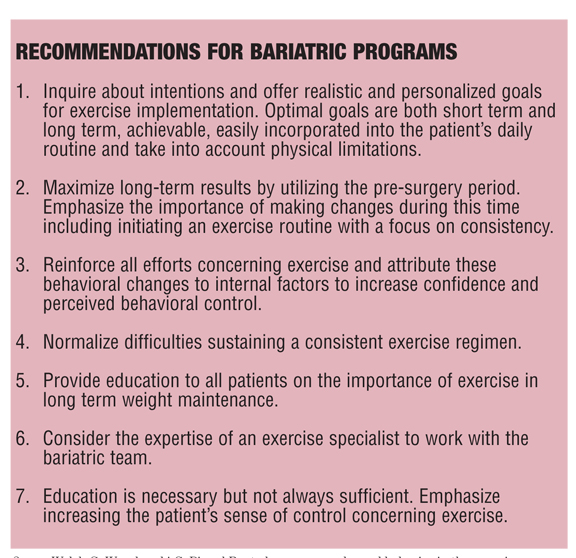
Recommendations for Bariatric Programs
Conclusion
A bariatric patient’s intention to follow recommendations for PA is the first step in a series of decisions toward achieving long-term implementation and successful maintenance of this behavior. The benefits of consistent PA have been discussed, as well as the obstacles and difficulties with patient adherence in this area. TPB offers a perspective regarding the examination of PA intentions through the variables of attitude, subjective norm, and PBC. It has been suggested that increasing a bariatric patient’s sense of control over his or her ability to lose and maintain the weight loss could be one means to increase PA adherence. This may be accomplished through both internal and external interventions, such as increasing confidence as well as providing an environment that supports goals and enhances PBC. Further research will be useful to examine strategies which can support increased PBC, as well as assistance with bariatric program development to examine patient’s existing PA intentions and the best means of translating these intentions into long-term success.
References
1. Livhits M, Mercado C, Yermilov I, et al. Exercise following bariatric surgery: systematic review. Obes Surg. 2010;20:657–665.
2. Welch G, Wesolowski C, Piepul B, et al. Physical activity predicts weight loss following gastric bypass surgery: findings from a support group survey. Obes Surg. 2008;18:517–524.
3. Evans RK, Bond DS, DeMaria EJ, et al. Initiation and progression of physical activity after laparoscopic and open gastric bypass surgery. Surg Innov. 2004;11(4):235–239.
4. Norman P, Conner M, Bell R. The theory of planned behaviour and exercise: evidence for the moderating role of past behaviour. Br J Health Psychol. 2000;5:249–261.
5. Bond DS, Evans RK, DeMaria E, et al. Physical activity and quality of life improvements before bariatric surgery. Am J Health Behav. 2006;30(4):422–434.
6. Petering R, Webb CW. Exercise, fluid, and nutrition recommendations for the postgastric bypass exerciser. Curr Sports Med Rep. 2009;8(2):92–97.
7. Elkins G, Whitfield P, Marcus J, Symmonds R, Rodriguez J, Cook T. Noncompliance with behavioral recommendations following bariatric surgery. Obes Surg. 2005;15:546–551.
8. Bond DS, Phelan S, Leahey TM, Hill JO, Wing RR. Weight-loss maintenance in successful weight losers: surgical vs non-surgical methods. Int J Obes. 2009;33:173–180.
9. McMahon MM, Sarr MG, Clark MM, et al. Clinical management after bariatric surgery: value of a multidisciplinary approach. Mayo Clin Proc. 2006;81(10,suppl):S34–S45.
10. Jakicic JM. Exercise in the treatment of obesity. Endocrinol Metab Clin North Am. 2003;32:967–980.
11. Hunt HR, Gross AM. Prediction of exercise in patients across various stages of bariatric surgery: a comparison of the merits of the theory of reasoned action versus the theory of planned behavior. Behav Modif. 2009;33(6):795–817.
12. Gatch CL, Kendzierski D. Predicting exercise intentions: the theory of planned behavior. Res Q Exerc Sport. 1990;61(1):100–102.
13. Ajzen I. Attitudes, Personality, and Behavior. Chicago, IL: Dorsey Press; 1988.
14. Courneya KS, Plotnikoff RC, Hotz SB. Social support and the theory of planned behavior in the exercise domain. Am J Health Behav. 2000;24(4):300–308.
15. Bond DS, Evans RK, DeMaria EJ, et al. A conceptual application of health behavior theory in the design and implementation of a successful surgical weight loss program. Obes Surg. 2004;14:849–856.
16. Schifter DE, Ajzen, I. Intention, perceived control, and weight loss: an application of the theory of planned behavior. J Pers Soc Psychol. 1985;49(3):843–851.
17. Ajzen I. Behavioral interventions based on the theory of planned behavior. http://www.people.umass.
edu/aizen/pdf/tpb.intervention.pdf. Accessed December 10, 2010.
18. Gollwitzer PM. Implementation intentions: strong effects of simple plans. Am Psychol. 1999;54:493–503.
19. Garber CE. Exercise as a complementary treatment in bariatric patients. Bariatric Times. 2007;4(1):28–30.
20. American College of Sports Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, Seventh Edition. Philadelphia: Lippincott, Williams & Wilkins; 2006.
21. Evans RK, Bond DS, Wolfe LG, et al. Participation in 150 min/wk of moderate or higher intensity physical activity yields greater weight loss after gastric bypass surgery. Surg Obes Rel Dis. 2007;3:526-530.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.







{kind=link}