
Bariatric Patient Postoperative Pain: A Potentially Promising New Route
by Susannah M. Wyles, MSc, MRCS; Sherif Hakky, MSc, MRCS; Ahmed R. Ahmed, BSc, FRCS; and Jonathan M. Cousins, BSc, FRCA
Dr. Wyles is Clinical Research Fellow, Department of Surgery and Cancer, St. Mary’s Hospital, Imperial College London, United Kingdom; Dr. Hakky, MSc, MRCS, is Laparoscopic Fellow, Department of Bariatric Surgery, Imperial Weight Centre, Imperial College Healthcare NHS Trust, London, United Kingdom; Dr. Ahmed, BSc, FRCS, is from the Department of Bariatric Surgery, Imperial Weight Centre, Imperial College Healthcare NHS Trust, London, United Kingdom; and Dr. Cousins, BSc, FRCA, is from the Department of Anesthetics, Imperial Weight Centre, Imperial College Healthcare NHS Trust, London, United Kingdom
Financial Disclosure: Ahmed R. Ahmed receives an educational grant from Ethicon Endosurgery. All other authors report no conflicts of interest relevant to the content of this article.
Abstract
Objective. Since early mobilization is a priority to minimize the number of avoidable complications, such as pneumonia or deep vein thromboses, good pain control is crucial for the postoperative bariatric patient. The aim of this study was to assess the value of the sub-lingual tramadol as a potentially beneficial alternative route of administration for the postoperative bariatric patient compared to the standard intravenous route. Design. Prospective study, with participants randomly allocated to receiving either sub-lingual or intravenous route tramadol. Setting. The study took place over a six-month period in a London hospital. Participants. Patients undergoing either a laparoscopic sleeve gastrectomy or gastric bypass were randomly allocated to either group. Measurements. Patients were asked to score their pain using a visual analog score both at rest and at movement before and after analgesia. These scores were analyzed using the Wilcoxon signed rank test (p significant if <0.05). Results. Sixteen patients were included in each group (intravenous route group: eight post sleeve, eight post bypass; sub-lingual group: five post sleeve, 11 post bypass). There was a demonstrated reduction in perceived pain both at rest and in movement. This was found to be statistically significant at rest for both routes (intravenous route p<0.0001, sub-lingual p<0.001), and in movement for both groups (intravenous route p<0.0001, sub-lingual p<0.001). On comparison of the variance between both modes, there was no statistically significant benefit of one route over the other (movement p=0.206, at rest p=0.321). Conclusions. This study shows that sub-lingual tramadol is as effective as intravenous tramadol as postoperative analgesia for the postoperative bariatric patient.
Introduction
“Bariatirc surgery is not cheap.” This is the common public misconception that any team working within this field battles with since many people do not appreciate the long-term health, economic, and patient benefits of bariatric surgery.[1] In the current Western economic climate, justifying the need to perform these “avoidable” operations is becoming more challenging with cuts and healthcare provision prioritization taking place.[2] Yet, with the worldwide number of patients with obesity continuing to rise, and given the knowledge that surgery is the best long-term solution for many of the obesity-related comorbidities, the surgery must continue.[3,4] The cost of surgery comes not from just the actual operation itself, but also the hospital stay, medications, and complications surrounding the surgery.[5] Anything that can minimize these costs without compromising patients should be carefully considered, particularly if it brings additional benefit to the patients.
Early mobilization in the postoperative bariatric patient helps minimize the number of potentially avoidable complications, such as pneumonia or deep vein thromboses, and can be facilitated by good pain control.[6–8] Administering effective pain control in postoperative bariatric patients can be difficult and carries additional risks for several reasons including the following: 1) obtaining intravenous (IV) access is often challenging in patients with a high body mass index (BMI), especially for junior staff, and IV administration of medications on a standard surgical ward have been associated with errors that can occur in both their preparation and administration;[9] 2) drug administration via the intramuscular route in this group of patients is often unachievable due to an excess of subcutaneous tissue; and 3) the use of some classes of analgesics might be contraindicated (e.g., the use of nonsteroidal anti-inflammatory drugs [NSAIDs]).
The aim of this study was to assess the value of the sub-lingual (SL) route of delivery of tramadol as a potentially beneficial alternative route of administration of this analgesia.
Methods
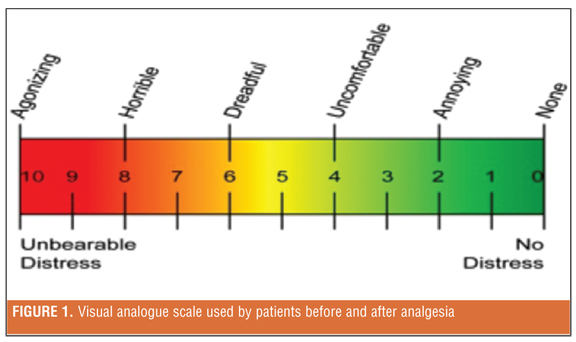
In late 2008, over a six-month period within a single-surgeon unit in a London hospital, patients who underwent either a laparoscopic sleeve gastrectomy (SG) or Roux-en-Y gastric bypass (RYGB) were selected for the study. Patients were randomly allocated to each group (SG and RYGB), irrespective of previous analgesia use, comorbidities, or subsequent complications. For the first three months of the study, patients were prescribed 100mg IV tramadol, six hourly for the first 24 hours postoperatively, which was given in addition to the concurrent administration of six hourly 1g IV paracetamol. This was the standard postoperative protocol for the bariatric surgical unit. In the subsequent three months, the route of tramadol administration was changed to SL. Additional analgesia was available if requested by the patients. After this, physicians switched all patients to regular oral analgesics. During the first 24 hours postsurgery, patients were asked to score their perceived pain using a 10-point, visual, analog scale coupled with a descriptive adjectival scale (Figure 1). Pain scores were given both at rest and in movement before and one hour after analgesia administation. The “before” score was given prior to the patients’ morning analgesia on Day 1 post surgery, which corresponds to 12 to 20 hours postsurgery, depending on the time of their surgery the day before. This was to ensure that there was no residual benefit from the analgesics used intraoperatively and immediately postoperatively in recovery. Data were analyzed using Wilcoxon signed rank nonparametric test given the small sample size within each group (SPSS v.18 [p=significant if <0.05]).
The Results
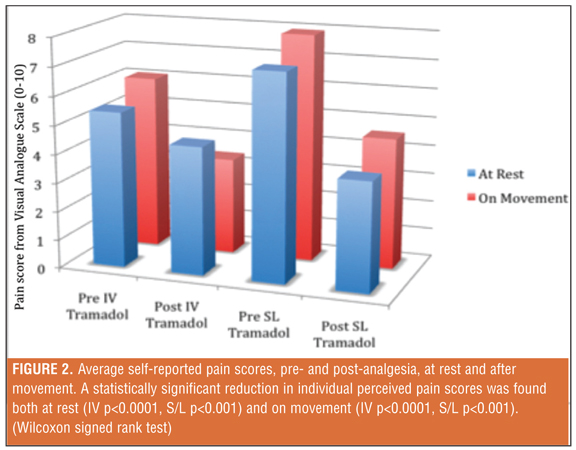
Twenty-two patients were recruited to each group. Several patients had to be excluded from the study due to the prescription of codeine rather than tramadol (five patients) and the failure to complete the visual analog scales both before and after analgesia (incomplete data, seven patients). Therefore, data were only analyzed for 16 patients in each group. For the IV group, eight underwent SG and eight RYGB. For the sub-lingual group, five underwent SG and 11 underwent RYGB. Wilcoxon signed rank test revealed a demonstrable reduction in individual perceived pain scores both at rest and in movement. This was found to be statistically significant at rest for both routes (IV p<0.0001, SL p<0.001) and in movement for both groups (IV p<0.0001, SL p<0.001). In comparison of the variance between both modes, there was no statistically significant benefit of one route over the other (pain in movement p=0.206, pain at rest p=0.321) (Figure 2). No additional analgesia was requested, and, on occasion, the analgesia prescribed was refused. The verbal nausea score ranged between 0 to 2 out of 10.
Discussion
This study shows that SL tramadol can reduce pain as effectively as the more usual IV route in the postoperative bariatric patient.
Pain control for bariatric patients is often difficult and the combination of drugs can be a challenge for anesthesiologists. There are several disadvantages associated with most of the analgesic drug groups that are especially pertinent to these patients. For example, the use of COX-2 inhibitors should be exercised with caution in this group of patients given their increased risk for ischemic heart disease and cerebrovascular disease, especially if a patient has noninsulin-dependent diabetes.[10] COX-2 inhibitors can be expensive[11] and most bariatric surgeons prefer not to administer NSAIDs due to their association with bleeding and marginal ulcer development.[12] Known side effects of codeine are cough suppression and constipation.[13–15] These can both become problematic in the postoperative state since bariatric patients are already at an increased risk of atelectasis, chest infection, and retained secretions. Furthermore, constipation can become a difficult symptom, particularly after RYGB, even when the patients are not prescribed codeine. The use of opioids is also difficult given lipophilia and reduced circulatory half life. Patient-controlled analgesics should be carefully considered before being set up, especially if fentanyl based.[11] Epidurals have also been found to be an independent risk factor for postoperative oxygen desaturation.[16]
Tramadol is not without complications or side effects, but when used in combination with regular paracetamol, patients reported significantly less pain at rest and minimal nausea when it was administered either IV or SL. This may have important implications. First, the cost of analgesic medicine can be reduced ten fold for each postoperative bariatric patient undergoing either RYGB or a sleeve gastrectomy. For example, in the United States, the cost per 100mg IV tramadol is approximately $3.50, compared with $0.36 per 100mg SL.[11,17] Although these figures are small, when projected annually the benefits can be seen. Second, removing the need for additional injections is a bonus for the patient; it may reduce some of the known risks of drug error and also mitigate potential injury from either the sharp of the needle or the glass of the drug vial to the administrator.[9] Using the SL route also prevents the medicine from being administered into the wrong tissue plane, and therefore assures a more certain dosage. Removing the need to prepare the medication may also help reduce the ward nursing staff’s workload. Third, irrespective of the operation performed or the previous comorbidities or regular analgesic use, the SL route tramadol performed as well as the IV route, and suggests that tramadol and paracetamol are a good standard baseline combination of analgesics for all patients.
Although it has been recently shown that there are some patient factors that do help predict analgesic requirements, this study provides a reminder that there are further suitable readily accessible routes for delivery of pain relief that should perhaps be considered before the hasty set up of epidurals or patient-controlled analgesia (PCA).[18] The results suggest that the pre-analgesia pain scores for those patients on SL tramadol are higher. This may simply be due to the fact that more people had RYGB compared to those patients within the IV tramadol group. Alternatively, it may be associated with the bioavailability of SL tramadol; it could be that the analgesia wears off more quickly before the next dose compared to via the IV route. However, there is little published evidence in the literature, and there is a need for further comparative pharmokinetic human studies.[19,20] Either way, effectiveness of both routes is demonstrated as each case acts as an internal control.
There are limitations to this study. The small sample size prevents a more detailed analysis. Given the time of maximal plasma concentration (Tmax) of oral tramadol is 120 minutes, this perhaps would have been a more appropriate time to collect the postanalgesic scores.[20] Furthermore, only a single pre- and post-analgesia score was taken for each patient at rest and then after movement, which prevents any trends or patterns to the postoperative pain pathway from being analyzed.
Conclusion
This study shows that SL tramadol is as effective as IV tramadol as postoperative analgesia for the postoperative bariatric patient. It should be considered as a valuable alternative, particularly as each dose is 10 times cheaper, it can be taken without water, and administration is potentially less time consuming for the nursing staff.
References
1. Royal College of Surgeons. http://www.rcseng.ac.uk/news/obesity-surgery-pays-for-iteself-in-12-months-says-new-report/?searchterm=obesity. Accessed September 30, 2010.
2. Campbell D. Call for more obesity surgery to cut benefits and NHS bills. The Guardian. September 7, 2010 http://www.guardian.co.uk/society/2010/sep/07/obesity-surgery-gastric-bypass. Accessed September 30, 2010.
3. Obesity. World Health Orginization Regional Office for Europe. http://www.euro.who.int/en/what-we-do/health-topics/diseases-and-conditions/obesity. Accessed September 30, 2010.
4. Nguyen NT, Root J, Zainabadi K, et al. Accelerated growth of bariatric surgery with the introduction of minimally invasive surgery. Arch Surg. 2005;140(12):1198–1202; discussion 203.
5. Picot J, Jones J, Colquitt JL, et al. The clinical effectiveness and cost-effectiveness of bariatric (weight loss) surgery for obesity: a systematic review and economic evaluation. Health Technol Assess. 2009;13(41):1–190, 215–357, iii–iv.
6. Nguyen NT, Cronan M, Braley S, et al. Duplex ultrasound assessment of femoral venous flow during laparoscopic and open gastric bypass. Surg Endosc. 2003;17(2):285–290.
7. Inabnet WB DE, Ikramuddin S. Laparoscopic bariatric surgery. USA: Lippincott Williams and Wilkins; 2005.
8. Ogunnaike BO, Jones SB, Jones DB, et al. Anesthetic considerations for bariatric surgery. Anesth Analg. 2002;95(6):1793–1805.
9. Taxis K, Barber N. Ethnographic study of incidence and severity of intravenous drug errors. BMJ. 2003;326(7391):684.
10. Roumie CL, Mitchel EF, Jr., Kaltenbach L, et al. Nonaspirin NSAIDs, cyclooxygenase 2 inhibitors, and the risk for stroke. Stroke. 2008;39(7):2037–2045.
11. Mehta DK. British National Formulary (BNF) 54: September 2007 (v. 54). London:Pharmaceutical Press; 2007.
12. Jordan JH, Hocking MP, Rout WR, Woodward ER. Marginal ulcer following gastric bypass for morbid obesity. Am J Surg. 1991;57(5):286–288.
13. Wood JD, Galligan JJ. Function of opioids in the enteric nervous system. Neurogastroenterol Motil. 2004;16 Suppl 2:17–28.
14. Galligan JJ, Vanner S. Basic and clinical pharmacology of new motility promoting agents. Neurogastroenterol Motil. 2005;17(5):643–653.
15. De Schepper HU, Cremonini F, Park MI, Camilleri M. Opioids and the gut: pharmacology and current clinical experience. Neurogastroenterol Motil. 2004;16(4):383–394.
16. Siriussawakul A, Mandee S, Thonsontia J, et al. Obesity, epidural analgesia, and subcostal incision are risk factors for postoperative desaturation. Can J Anaesth. 2010;57(5):415–422.
17. Currency converter. http://coinmill.com/GBP_USD.html. Accessd September 30, 2010.
18. Weingarten TN, Sprung J, Flores A, et al. Opioid requirements after laparoscopic bariatric surgery. Obes Surg. 2010 Jun 19. [Epub ahead of print]
19. Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet. 2004;43(13):879–923.
20. Gibson TP. Pharmacokinetics, efficacy, and safety of analgesia with a focus on tramadol HCl. Am J Med. 1996;101(1A):47S–53S.
Category: Original Research, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}