
New Column! Nutritional Considerations in the Bariatric Patient. This month: Pica: An Ancient Disorder with Modern Casualties
Nutritional Considerations in the Bariatric Patient
Pica: An Ancient Disorder with Modern Casualties
This Month’s Contributor: Liz Goldenberg, MPH, RD, CDN
Ms. Goldenberg is a nutritionist at New York Presbyterian Hospital, Weill Cornell College of Medicine of Cornell University, Department of Surgery, New York, New York.
Bariatric Times. 2010;7(11)22–23
This ongoing column is dedicated to providing evidence-based bites of information for the clinician on nutritional considerations in the bariatric patient. Introduction
There are numerous health benefits to undergoing weight loss surgery; however, these operations can also increase patients’ risk for developing a number of nutrient deficiencies. Iron deficiency anemia (IDA) is prominent among the deficiencies that may develop. Pica is a disorder that is commonly linked with IDA. The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) defines pica as “the persistent eating of nonnutritive substances for a period of at least one month, without an association with an aversion to food.” Compulsions to eat laundry starch, ice (termed pagophagia), cigarette ash, dirt or clay (both termed geophagia), as well as other unusual nonfood substances, have been documented. While its pathogenesis is still not completely understood, theories of mineral deficiency, such as iron and zinc, are most commonly cited as causing pica, while supplementation with iron appears to rapidly relieve the odd cravings.[1]
Pica is believed to come from the Latin word for the magpie bird that eats both foods and nonfoods indiscriminately. Pica of dirt and clay was known to the Greeks and the Romans and was recorded as early as the 13th century. Pica was first noted in the medical literature in the 16th century, describing clay-eating in pregnant women and in children.[2]
Patients who have undergone operations that have a malabsorptive component, such as Roux-en-Y gastric bypass (RYGB) and biliopancreatic diversion (BD), with or without duodenal switch, are at increased risk for developing IDA and subsequently pica. The following is a list of reasons that may contribute to IDA and pica:[3]
• Intake of iron-rich foods, such as meats and fortified grains, are often limited after surgery.
• Decreased hydrochloric acid production may occur in the stomach.
• Food and supplements bypass iron absorption sites in the duodenum and proximal jejunum.
• Fewer receptors are available to a) transport iron and b) reduce iron to its more absorbable ferrous form.
• Nonadherence with nutrient supplements may occur.
• Approximately one-half of weight loss surgery patients are women of child bearing age (menstrual losses and pregnancy increase risk for IDA and pica).[4]
There are some revealing case studies[1,5,6] that describe pica in patients who have undergone weight loss surgery, primarily after RYGB. Seemingly bizarre reports tell of patients with intense ice cravings, who ingest more than 100 ounces of ice daily. One paper described a female patient who purchased two snow-cone machines, one for home and another for work. Another tells of a woman who likened her ice craving to a drug addiction. She once found herself driving to purchase a bag of ice in the middle of the night, and needing to break open the bag on the way to her car. There are other cases of women ingesting such things as used coffee grinds and 40 to 50 Tums® tablets (containing 10,000mgs of calcium, which inhibits iron absorption) daily. A recent case report by Moize et al[6] describes periodontal disease including dental fractures and the absence of pieces of teeth as an irreversible consequence of pica after RYGB.
While some of the case reports are of women who had pica tendencies prior to surgery, (e.g., during pregnancy or as a child growing up a rural community where pica is more common),[1] it is important to note that there are also instances of new diagnoses. Iron deficiency is the most common nutritional deficiency worldwide, affecting 9 to 16 percent of adult women in the general population. Studies have shown that 20 to 49 percent of RYGB patients develop a deficiency of this mineral.[3]
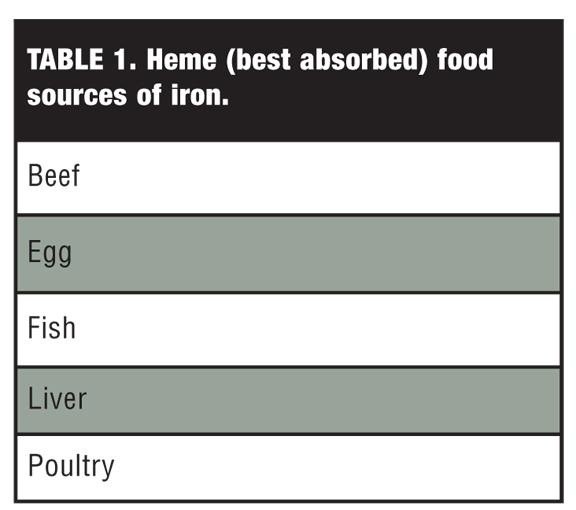
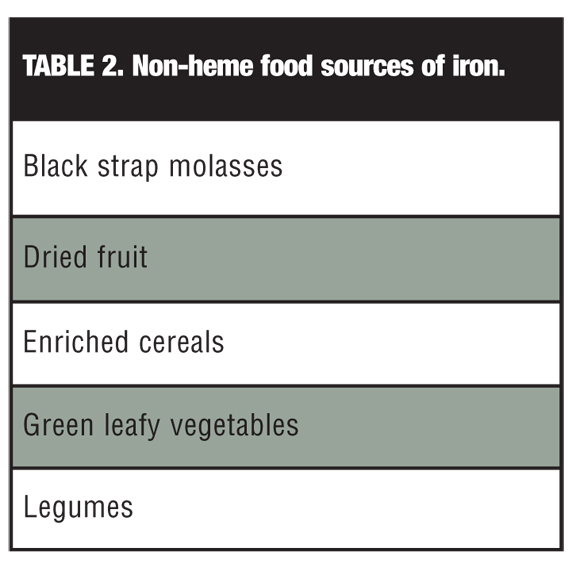
There are a number of methods that can help to prevent, or treat, IDA. Patients should be encouraged to consume iron-rich foods and foods with vitamin C, such as oranges and tomatoes, which improve the absorption of non-heme iron from foods (Table 1 and Table 2). Note that absorption of non-heme iron is impaired by phytates, such as bran products, cocoa, nuts, and by phenolic compounds, such as tea, coffee, and calcium-containing foods or supplements. It has been suggested that low-risk patients, including men and postmenopausal women, follow a daily regimen that includes two complete multivitamins, collectively providing 36mg of iron.[3] The American Association of Clinical Endocrinologists published guidelines recommending that patients undergoing malabsorptive surgery should take one to two multivitamins with multitrace elements plus an additional 40 to 65mg elemental iron daily.[7] An older paper by Brolin et al[8] suggests an even higher prophylactic iron dose for menstruating women. To prevent anemia, the authors recommend supplementation with two 320-mg ferrous sulfate tablets (providing 100mg of elemental iron) daily.[8] In patients who do not respond to diet and oral supplements, intravenous (IV) iron infusion in the form of iron-dextran or iron-sucrose should be considered.[9] Lastly, it may be helpful for women to reduce their menstrual losses by taking oral contraceptive agents.
For more information on IDA and pica, the author recommends the ASMBS Allied Health Nutritional Guidelines for the Surgical Weight Loss Patient published in Surgery and Obesity Related Diseases.[3]
References
1. Kushner RF, Gleason B, Shanta-Retelny V. Reemergence of pica following gastric bypass surgery for obesity: a new presentation of an old problem. J Am Diet Assoc. 2004;104(9):1393–1397.
2. Parry-Jones B, Parry-Jones WL. Pica: symptom or eating disorder? A historical assessment. Br J Psychiatry. 1992;160:341–354.
3. Aills L, Blankenship J, Buffington C, et al. ASMBS allied health nutritional guidelines for the surgical weight loss patient. Surg Obes Relat Dis. 2008;4(5 Suppl):S73–S108. Epub 2008 May 19.
4. Maggard M, Li Z, Yermilov I, et al. Bariatric Surgery in Women of Reproductive Age: Special Concerns for Pregnancy. Evidence Report/Technology Assessment No. 169. (Prepared by the Southern California Evidence-based Practice Center under Contract No. 290-02-003). Rockville, MD: Agency for Healthcare Research and Quality; November 2008.
5. Kushner RF, Retelny VS. Emergence of pica (ingestion of non-food substances) accompanying iron deficiency anemia after gastric bypass surgery. Obes Surg. 2005;19(11):1491-5.
6. Moize V, Moize L, et al. Pica secondary to iron deficiency 1 year after gastric bypass. Surg Obes Relat Dis. 2010;6(3):316–318.
7. Mechanick JI, Kushner RF, Sugerman HJ, et al. American Association of Clinical Endocrinologists, The Obesity Society, and American Society for Metabolic and Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric surgery patient. Endocr Pract. 2008;14:1–83.
8. Brolin RE, Gorman JH, Gorman RC, et al. Prophylactic iron supplementation after Roux-en-Y gastric bypass: A prospective, double-blind, randomized study. Arch Surg. 1998;133:740–744.
9. Fujioka K. Follow-up of nutritional and metabolic problems after bariatric surgery. Diabetes Care. 2005;28:481–4.
Coming Up!
In the next installment of “Nutritional Considerations in the Bariatric Patient,” don’t miss Cognitive Problems in the Thiamin-deficient Post-bariatric Surgery Patient—January 2011
Category: Nutritional Considerations in the Bariatric Patient, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}