
Maintaining Dignity of Patients with Morbid Obesity in the Hospital Setting
This CE activity is expired.
by Shirley A. Thomas, RN, MPA, and Mary Lee-Fong, RN-C, MSN
Ms. Thomas is the nurse manager of the Vascular and GI Surgery and Telemetry Unit and Bariatric Consultant at UC Davis Medical Center in Sacramento, California. She serves on the National Association of Bariatrics Nurses Board. Ms. Lee-Fong is the assistant manager of the Vascular and GI Surgery and Telemetry Unit.
Funding: This CE-accredited article was supported by an educational grant from KCI.
Financial disclosure: Ms. Thomas and Ms. Lee-Fong report no conflicts of interest relevant to the content of this article.
Bariatric Times. 2010;8(4):20–25
Abstract
Bariatric patients have their own set of needs. If the healthcare professional is aware of these needs, it is more likely the bariatric patient will be treated with dignity. It is important for patients with obesity to be provided dignified care at all times. This article reviews proper caregiver education and training; fostering respectful communication using supportive language; developing bariatric protocols; providing size-appropriate furnishings, equipment, supplies and instruments; and having the right equipment at the right place and right time. In addition, the development of a bariatric team of experts to consult on mobility and care issues for these patients is paramount in promoting patient and staff safety and ensuring the best possible dignified care for patients with morbid obesity.
Introduction
Obesity is rapidly becoming the most chronic and serious epidemic and health problem of this century.[1] According to the National Health and Nutrition Examination Survey, more than two-thirds of adults in the United States are overweight or obese.[2] The healthcare setting is experiencing an increase in this bariatric patient population each year. Bariatric patients have their own unique set of needs. If the healthcare professional has an awareness of these needs, it is more likely that the bariatric patients will be treated with dignity. It is important for patients with obesity to be provided dignified care at all times. This article reviews proper caregiver education and training; fostering respectful communication using supportive language; developing bariatric protocols; providing size-appropriate furnishings, equipment, supplies, and instruments; and having the right equipment at the right place and right time. In addition, the development of a bariatric team of experts to consult on mobility and care issues for these patients is paramount in promoting patient and staff safety and ensuring the best possible dignified care for patients with morbid obesity.
With the increasing rate of obesity in patients in the hospital setting, it is important to maintain the dignity of the bariatric patient. Obesity has increased from 14.4 percent to 30.9 percent from 1976 to 2000.[3] In this article, the words obese and bariatric will be used to describe the patient population. The word obesity originates from a Latin term meaning “fattened by eating.” Bariatrics refers to the practice of healthcare relating to the treatment of obesity and associated conditions.[4] Caring for the bariatric patient can be challenging and healthcare professionals need education, proper equipment, and established protocols to enable them to give the best possible dignified care to patients with obesity. It is true that the healthcare professional may have a personal bias regarding obesity and concerns about receiving injuries while providing care to the bariatric patient.[4] This is why it is essential for the healthcare setting to have systems in place to identify and meet the needs of bariatric patients.
Providing Bariatric Care with Dignity
According to the Obesity Action Coalition (OAC) an estimated 93 million Americans have obesity, and this number is predicted to climb to 120 million within the next five years.[5] Studies show that this disease and its impact on one’s mobility and quality of life can cause bias, discrimination and social stigmas (Figure 1).[1,4,6] Bariatric patients are not always treated with the dignity that nonobese patients may receive. Dignity is a term used in moral, ethical, and political discussions to signify that a being has an innate right to respect and ethical treatment.[7] Treating bariatric patients with a lack of dignity in the hospital setting might cause them to be reluctant to seek medical care because of feelings of embarrassment and shame.[1,8,9]
According to Bejciy-Spring,[1] anti-fat or weight bias, a devaluing of a person based on excess body weight, is considered one of the most complicated social phenomena, and has been described as the last safe domain of discrimination and prejudice in the United States. There is clear, consistent evidence through research that individuals with obesity experience discrimination in family, social, education, and employment settings.[1]
Studies also show that several categories of healthcare professionals, including physicians, medical students, nurses, dietitians, and behavioral health professionals, share the same attitudes of obesity and weight bias and discrimination as the general public.[1,4,8,9]
Brownell and Puhl[9] report that in a number of studies several healthcare professionals have negative attitudes toward patients with obesity.[9] These studies reveal that some healthcare professionals hold beliefs that patients with obesity lack self control, are lazy, and have character flaws causing them to be nonadherent in attempting to lose weight. Until the majority of healthcare providers understand the challenges of obesity and the multifactorial causes of obesity, these patients will continue to experience discrimination, bias, limited access to healthcare, and isolation.[1,3,4,6]
In her book The Challenges of Caring for the Obese Patient, Gallagher[4] states, “Even the most compassionate caregiver may be reluctant to provide adequate care [to a patient with obesity] because of the threat of caregiver injury. The fear of injury is realistic and, combined with the failure to provide satisfactory care to a complex patient, causes further perpetuation of discrimination toward the obese patient.” Healthcare professionals should consider taking some time for self reflection to examine how they feel about patients with obesity and educate themselves on how to provide care for bariatric patients without bias and discrimination.
Using Communication to Provide Dignified Bariatric Care
A key element in providing dignified care is building a relationship with the patient through compassionate communication. Rowen[10] describes relationship-based care as “when the patient and family feel our respect through our protection of their dignity, privacy and well being.” Providing proper education on the multifactorial causes of obesity and training on how to communicate with sensitivity can build a trusting relationship and connection between the healthcare provider and the bariatric patient.
Respectful and nonbiased communication can be achieved by using supportive language. Martinez[6] states, “Our patients are not ‘morbidly obese patients;’ rather, they are patients who suffer from morbid obesity. We don’t say ‘the ovarian cancer woman,’ so why do we say ‘the morbidly obese woman’?”[6] It is important to have an awareness about the words we choose when we are having a discussion with a bariatric patient. Some words that could be substituted when communicating with or about the bariatric patient can be found in the Table 1.[11]
Imagine that you have obesity and the nurse comes into your hospital and says, “Are you over 300 pounds because our scale won’t go up that high.” A more reasonable approach to this situation may be for the nurse to anticipate in advance that the patient would need a scale with a higher weight capacity, know how to use the scale properly, and provide privacy during the weighing so the weighing process can be a more dignified experience. In the past, at a time when patient scales were only available with a weight capacity of 350 pounds, bariatric patients over 350 pounds were weighed on the scales located on the loading dock of hospitals. This was very humiliating and embarrassing to the patients and clearly was not a dignified process. Now scales are available that have a weight capacity of 750 to 1,000 pounds..
Development of Bariatric Protocols
Another key element in providing dignity to the bariatric patient is the development of bariatric protocols. Protocols provide guidelines and standards that ensure consistency in the delivery of care. It is important to develop protocols for all bariatric patients, not just those having weight loss surgery. Wright and Bauer[12] state, “Development of an organizational-wide protocol specifically designed to meet the needs of all patients will facilitate the provision of safe and dignified care for both patient and caregiver.” Protocols should do the following:
1. Provide healthcare professionals with training and education on how to use bariatric equipment
2. Identify when assistance is required with mobility
3. Provide the proper equipment (blood pressure cuffs, and furniture) to give the bariatric patient the best possible care while respecting their dignity.
McGinley and Burke[13] have a report on a task force from the National Association of Bariatric Nurses (NABN) that developed recommendations for establishing a bariatric protocol for the safe handling of the bariatric patient. The protocol is evidence based and can be used by all institutions, including those not performing bariatric surgery. Recommended elements of the protocol are as follows:[13]
1. Be proactive by identifying a plan based on the patient’s needs “door to door.”
2. Establish protocols and algorithms involving a multidisciplinary team for safe handling, equipment, number of staff, and preoperative and postoperative needs.
3. Develop a safe lifting policy.
4. Insist on multidisciplinary teamwork and effective communication.
5. Adopt an effective staff education program.
6. Utilize proper assistive equipment.
Bariatric protocols are already being implemented in some healthcare institutions. One such protocol explains how to meet the physical needs of the bariatric patient by promoting clinical safety and dignity.[12] This protocol begins on admission with the patient’s weight and height and estimation of level of dependency. Skin complications and assessment of the type of bariatric equipment needed are also noted. In this protocol, consultations and referrals are generated to the wound nurse, physical therapist, occupational therapist, social worker, dietician, and the bariatric consultant.[12,14]
Arzouman[15] developed a bariatric protocol template recommending that bariatric patients have a private room.[15] The protocol suggests that an inventory list of the hospital’s bariatric equipment be added as a resource along with the location, weight capacity, and manufacturer. The protocol should identify the weight capacity and width of the bed for the bariatric patient.
Unfortunately, there are times in the healthcare setting that protocols have not been put into place until after harm has reached the bariatric patient. The Joint Commission (JC) now requires all acute care hospitals to perform a failure mode and effect analysis (FMEA) regularly. This analysis has proven to be an effective method of minimizing errors in the healthcare community.[16] The FMEA process can be used as a template for a protocol to care for the bariatric patient. The FMEA process contains the following seven steps:[16]
Step 1. Select and define a process. Some processes may include equipment use, sensitivity training, patient education, and structural challenges.
Step 2. Assemble a multidisciplinary team. A team ahould consist of members with different viewpoints of the patient care experience.
Step 3. Clarify the issues using graphical display of the process. Use a timeline of the process from entry into the medical setting until discharge. This could include transport difficulties with doors, beds, ramps, and staff difficulties with ergonomic, safety, and sensitivity issues.
Step 4. Identify and prioritize failure points.
• What can go wrong?
• If it goes wrong, how bad might it be (severity)?
• How likely is it to go wrong (frequency)?
• Are there systems in place to detect if something has gone wrong?
Step 5. Perform a root cause analysis of significant failure points.
• What structural, staff, patient, or equipment issues are involved?
• What would have to go wrong for a failure like this to happen?
• Why is the failure not recognized more quickly?
• Are particular personnel more likely to experience this failure?
Step 6. Plan for improvement. Be proactive and eliminate the failure from happening. Make it easier for staff to do the right thing. Identify failures early and implement corrective action.
Step 7. Monitor and evaluate the chosen strategies. Outcome measurements are best, such as pressure ulcers caused by equipment or tracking the percentage of staff who attend training. It is important for a committee or individual to take responsibility for the process.
After using the FMEA process model, potential failure points can be more easily identified to pinpoint areas for improvement. After becoming knowledgeable of the protocols, the healthcare provider can communicate with all disciplines involved in the care for the bariatric patient, which will help provide the best care possible while preserving the dignity of the patient.
Considerations for Essential Bariatric Equipment, Furnishings, and Supplies
Providing the essential and right equipment at the right place and time is crucial for promoting patient and staff safety and ensuring dignity for the bariatric patient. Gallagher[4] describes the following four key elements to ensuring dignity and sensitivity in the healthcare setting:[4]
1. Establishing a multidisciplinary bariatric task force to address ongoing issues, quality of care, and ideas
2. Developing criteria-based protocols based on the patient’s weight, body mass index (BMI), body width, and clinical condition
3. Educating and training staff on competencies and skills set;
4. Developing outcome measurements.
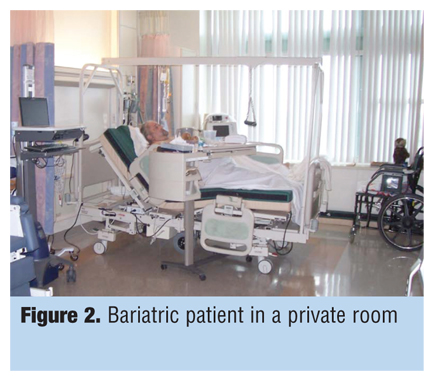
Resources for recommendations on bariatric equipment, furniture, and instruments have increased over the past few years. Detailed descriptions and photographs of various types of equipment needed for the care of bariatric patients are available to provide guidance to healthcare professionals (Figure 2, Figure 3, Figure 4, and Figure 5).[1,3,4,13–15,17–21] Table 2 is a composite of recommended bariatric equipment based on the literature search.[1,3,4,13–15,17–21]
Facility design considerations should include concepts that incorporate dignity. In an original inquiry brief, The Advisory Board Company19 found that administrators had made several accomodations for bariatric patients, including converting double-patient rooms to single-patient rooms; adjusting doorways to be wider; adding bariatric equipment, including blood pressure cuffs of various sizes; making showers wheelchair accessible; and changing toilets from wall mounted to floor mounted. If the institution is unable to change the toilets to floor mounted, an option may be to use a 800- to 1,000-pound capacity bedside commode placed over the wall mounted toilet (Figure 3a). Magnetic resonance imaging (MRI) equipment, computerized tomography (CT) scanners, and fluoroscopy equipment were upgraded to increased weight capacity. Waiting areas seating was changed to wider chairs.
Physical space and lack of clutter are important considerations in reducing the risk of falls (Figure 2). Hallways and doorways should accommodate wider and longer equipment.[17–19] Appropriate-sized visitor chairs may be necessary to accommodate the patient’s family, who may have obesity.
It is important to know the weight capacities, physical dimensions, and limitations of all bariatric equipment (e.g., beds, chairs, wheelchairs, and toilets). The hospital should provide the appropriate education on the bariatric equipment and bariatric sensitivity training for all staff members who work with bariatric patients. This is important in establishing an environment that promotes dignity in the care of bariatric patients. Bejciy-Spring’s[1] recommendations are that appropriately sized equipment, such as beds, wheelchairs, toilets, beside commodes, chairs, exam tables, and lifting devices, be consistently and readily available. Patients should have the appropriate gowns, robes, bed linens, and examination drapes. Healthcare providers should pay special attention to not exposing the patient and preserving privacy by closing the door or privacy curtain.[1] The healthcare professional should address the safety needs of the patients’ family members, who may also have obesity. This could include providing a variety of seating options, which will reduce undue attention and embarrassment.
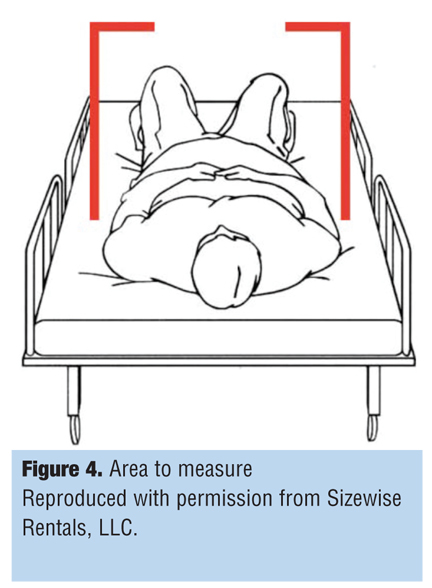
Ideally, the bariatric bed should be available upon the patient’s arrival to the emergency department, operating room, or patient care unit. Arrangements can be made with bariatric equipment rental companies to store extra beds on site at the facility so they can be easily accessible and the patient does not have to wait. In the emergency department, placing the bariatric patient on a bariatric bed immediately is more comfortable than a gurney, and the patient can easily raise the head of the bed, if needed. To determine the appropriate width for the bariatric bed, measure the patient elbow to elbow, or at the widest point while the patient is supine, if tolerated, so as to prevent pressure injuries from the side rails on the arms, legs, or hip (Figure 4). Some bariatric beds with mattress overlays do not have back-up batteries, and the mattress deflates 100 percent for transport when the bed is unplugged. This results in the patient resting on the bed frame during the transport, causing pressure-related skin injuries. An inflatable air mattress can be used on these types of beds to reduce the risk of skin injuries during transport. If indicated, provide a bariatric low-air-loss overlay mattress for prevention or treatment of pressure ulcers; treatment of severe or extensive burns, flaps, and grafts; pain management; or to aid in circulation.
Resources for mobilizing the bariatric patient should be available during all shifts, not just primarily during the day or evening shifts. The night shift nurses are at higher risk for injury when resources are minimized.
Providing privacy when weighing patients is key to ensuring dignity. Consider locating the scale where the weight cannot be overheard. Turn the scale so the weight cannot be viewed by others. Consider a curtained or secluded area.
Bariatric patient gowns should have a circumference that allows the gown to overlap and close completely in the back. The armholes of the gowns should be wide so as not to restrict the arms. Robes and slippers should come in a variety of sizes.
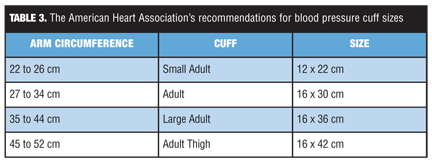
When taking vital signs, the blood pressure measurement may be higher when the blood pressure cuff is too small.[22–24] Marks and Groch22 described the criteria for the “ideal” cuff, stating that it “should have a bladder length that is 80 percent and a width that is at least 40 percent of arm circumference (i.e., a length-to-width ratio of 2:1).”[22] It is recommended that if a correct size cuff is not available, the clinician use a regular-sized cuff on the forearm or lower leg.[25] The American Heart Association’s recommendations for blood pressure cuff sizes are described Table 3
.[23]
In the case of a pregnant bariatric patient in labor who has thick skin folds, using an external fetal monitor may make it difficult to get accurate readings on fetal heart rate and strength of contractions. In this situation, consider applying an internal fetal monitor if indicated.
In the perioperative setting, Hunt[26] described comprehensive recommendations to address patient safety and caregivers’ use of appropriate terminology. Operating room tables with a weight capacity of up to 1,000 pounds are available. Standards and protocols are endorsed as necessary for resource and training. The weight capacity of equipment should be visible but not prominent to maintain patient dignity.[26]
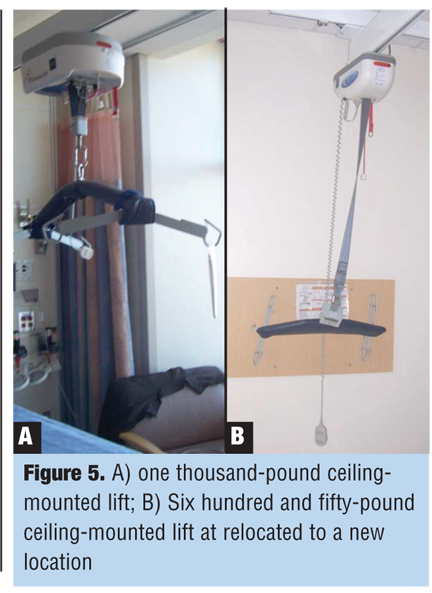
Ceiling-mounted lifts are being considered by healthcare institutions for retrofitting in existing patient rooms and for new construction. Getting nursing staff’s input regarding the location is important to ensure the lift is placed in the best possible location. Choosing the best ceiling-mounted lift for the specific bariatric patient needs depends on having adequate space. Our institution installed our first 1,000-pound capacity, ceiling-mounted lift in 2009. After it was completely installed, we realized that it was hanging too low and partially blocked the space over the patient’s bed (Figure 5). It prevented the caregiver from accessing the patient and the headwall unit with oxygen and suction. It was later replaced with a smaller motor and the staging location was changed to the opposite side of the room for a better fit. After these adjustments were made, it no longer interfered with patient access (Figure 6).
Use caution with air mattresses and mattress overlays on bariatric beds. At times, the mattresses cause the overall height to be too high so side rails are not protecting the patient, which can be a fall-risk issue. It also could make it difficult to reach the patient while turning. Attention should be paid to the location of the height of the bed in relation to the caregiver’s pelvis when reaching to turn the patient.
Dignity When Turning or Moving a Bariatric Patient
Similar to the surgical pause or JC’s Program Speak Up™, [27] there should be a conscious and deliberate discussion regarding the safest means and best equipment to utilize before moving a patient with morbid obesity. At University of California Davis Medical Center (UCDMC), the multidisciplinary team first meets to discuss with the patient the safest method to move the patient, taking into consideration the patient’s desires and concerns. The team then discusses options away from the bedside as to not cause the patient undue anxiety about the process of getting out of bed. The bariatric consultant[14] leads the team, which includes the primary nurse, charge nurse, physical therapist, occupational therapist, lift technician, and lift technician supervisor. Once the safest and most dignified plan is identified, the team explains to the patient the details of the plan and again addresses any concerns the patient may have. See Sidebar “Maintaining Patient Dignity During a Turn or Move: A Success Story”
Lift teams are a practical and vital model for ensuring dignity for the bariatric patient. Nelson described justification, tools, strategies, implementation, and evidence to support lift teams.[3,4] Lift teams have reduced patient and staff injuries substantially, and the lift technicians at UCDMC are well educated in sensitivity training. Lift technicians are competent and well trained in the management of moving and lifting patients. Their kind, calm, and professional approach to the bariatric patient validates their compassion and willingness to be accommodating and flexible to meet the bariatric patient’s needs (Figure 6).
CONCLUSION
Ensuring dignity for the bariatric patient requires a comprehensive approach based on building relationships and trust through compassionate communication using supportive language. Education and training on the challenges of caring for the bariatric patient can begin to alter personal biases regarding obesity. The development of bariatric protocols can be an essential resource for the healthcare provider and the multidisciplinary team. Providing the size-appropriate furnishings, equipment, supplies, and instruments and having the right equipment at the right place and right time promotes efficiencies. In addition, the development of a bariatric team of experts is desirable to act as consultants on equipment, mobility, and care issues which may improve the bariatric patient’s confidence in staff.
References
1. Bejciy-Spring S. R-E-S-P-E-C-T: a model for the sensitive treatment of the bariatric patient. Bariatric Nursing and Surgical Patient Care. 2008;3(1):47–56.
2. Overweight and Obesity Statistics. United States Department of Human Services, National Institute of Diabetes and Digestive and Kidney Diseases. http//win.niddk.nih.gov/publications/PDFs/stat904z.pdf: pages 1–7. Accessed March 2, 2011.
3. Baptiste A. Safe bariatric patient handling toolkit. Bariatric Nursing and Surgical Patient Care. 2007;2(1):17–45.
4. Gallagher S. The Challenges of Caring for the Obese Patient. Edgemont, PA: Matrix Medical Communications; 2005.
5. Obesity Action Coalition. http://www.obesityaction.org/aboutobesity/overview.php. pages 1–7. Accessed March 1, 2011.
6. Martinez T. Conveying empathy: Why are we still struggling? Bariatric Times. 2009;(6):2–7.
7. Dignity. http://en.wikipedia.org/wiki/Dignity. pages 1–9. Accessed February 20, 2011.
8. Hurst S, Blanco K, Boyle D, et al. Bariatric implications of critical care nursing. Dimens Crit Care Nurs. 2004;23(2):76–83.
9. Brownell K, Puhl R. Stigma and discrimination in weight management and obesity. The Permanente Journal. 2003;7(3):21–23.
10. Rowen L. Living and breathing relationship-based care. Bariatric Nursing and Surgical Patient Care. 2007;2(3):159–160.
11. Supportive language. Adapted from the work of Linda Omichinshi, RD. http://www.cell
interactive.com/ucla/physcian_ed/supp_lang.html. Acessed March 1, 2011.
12. Wright K, Bauer C. Meeting bariatric patients’ care needs. J Wound Ostomy Continence Nurs. 2005;32(6):402–406.
13. McGinley L, Bunke J. Best practices for safe handling of the morbidly obese patient. Bariatric Nursing and Surgical Patient Care. 2008;3(4):255–260.
14. Thomas S, Rickabaugh B. Bariatric nurse coordinator: carving out a new role in bariatrics. Bariatric Nursing and Surgical Patient Care. 2008;3(1):63–72.
15. Arzouman J, Lacorva J, Balckett A, et al. Developing a comprehensive bariatric protocol: a template for improving patient care. Medsurg Nursing. 2006;15(1):21–26.
16. Cheung D, Maygers J, Khouri-Stevens Z, et al. Failure modes and effects analysis: minimizing harm to our bariatric patients. Bariatric Nursing and Surgical Patient Care. 2006;1(2):107–114.
17. Gourash W, Rogula T, Schauer P. Essential bariatric equipment: making your facility more accommodating to bariatric surgical patients. In: Schauer P, Schirmer B, Brethauer S, eds. Minimally Invasive Bariatric Surgery. New York: Springer Publishing Company; 2007:37–49.
18. Lloyd J. Patient handling technologies. In: Nelson A, ed. Safe Patient Handling and Movement. New York: Springer Publishing Company; 2006:89–103.
19. Andrade, S. Planning and design guidelines for bariatric healthcare facilitiies. American Institute of Architects Academy Journal. http://info.aia.org/nwsltr_print.cfm?pagename=aah_jrnl_20061018_award_winner. Accessed March 1, 2011.
20. Medical Care for Obese Patients. United States Department of Health and Human Services. 2007. United States Department of Health and Human Services, National Institutes of Diabetes amd Digestove amd Kidney Diseases. http://www.win.niddk.nih.gov/publications/PDFs/medcareobesebw.pdf. Accessed March 1, 2011.
21. Lautz D, Jiser M, Kelly J, et al. An update on best practice guidelines for specialized facilities and resources necessary for weight loss surgical programs. Obesity (Silver Spring). 2009;17(5):911–917.
22. Marks LA, Groch A. Optimizing cuff width for noninvasive measurement of blood pressure. Blood Press Monit. 2000;5(3):153–158.
23. Pickering T, Hall J, Appel L, et al. Recommendations for blood pressure measurement in humans and experimental animals. 2005. http://hyper.ahajournals.org/cgi/content/full/45/1/142. Accessed March 5, 2011.
24. Maxwell M, Waks A, Schroth P, et al. Error in blood-pressure measurement due to incorrect cuff size in obese patients. Lancet. 1982;2(8288):33–36.
25. Gallegher Camden S. Obesity: an emerging concern for patients and nurses. The Online Journal of Issues in Nursing. 2009;14(1):1–8.
26. Hunt D. Evaluating equipment and techniques for safe preoperative positioning of the morbidly obese patient. Bariatric Nursing and Surgical Patient Care. 2007;2(1):57–63.
27. Speak Up. http://www.jointcommission.org/assets/1/18/UP_Poster.pdf. Accessed March 5, 2011.
Category: Past Articles, Review
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Half of the program can not be visulized due to right sided ads. Unable to close or read.
thanks
You must extend your browser window by clicking and dragging the bottom right corner of your browser window down and to the right. This will move the ads over.