
Metabolic and Bariatric Surgery: New Insights Provide New Opportunities
Exclusive Series: The Metabolic Applied Research Strategy initiative
Part 7: Metabolic and Bariatric Surgery: New Insights Provide New Opportunities
by Jason L. Harris, PhD; Randy J. Seeley, PhD; and Lee M. Kaplan, MD, PhD
Bariatric Times. 2012;9(9):10–12
Abstract
The Metabolic Applied Research Strategy is a multi-year, multi-generational collaborative research program between the Massachusetts General Hospital, the University of Cincinnati, and Ethicon Endo-Surgery. Its focus is to interrogate and understand the physiologic and metabolic changes that occur after bariatric surgery (i.e., how bariatric surgery works to resolve conditions such as type 2 diabetes) with the goal of inventing new, less invasive, and less expensive treatments for patients suffering from obesity and its related health issues. In this article, which is the seventh and final in a series of articles published in Bariatric Times dedicated to the Metabolic Applied Research Strategy initiative, the authors discuss past and present understanding on why bariatric surgery works, its mechanism of action, and how these findings might help researchers, surgeons, and industry harness the remarkable effectiveness of bariatric surgery.
Jason L. Harris, PhD
Dr. Jason L. Harris is a Principal Engineer leading Metabolic Applied Research Strategy co-invention and product development efforts at Ethicon Endo-Surgery, a Johnson and Johnson company. Since 2006, he has been exploring novel treatment approaches for patients suffering from the effects of metabolic disease. His primary focus is applying insights from basic and applied research efforts to develop improved therapies and predictive tools for the treatment of this disease.
Randy J. Seeley, PhD
Dr. Randy J. Seeley is Professor of Medicine and holds the Donald C. Harrison Endowed Chair at the University of Cincinnati College of Medicine. In 2009, Dr. Seeley was appointed as the Director of the Cincinnati Diabetes and Obesity Center (CDOC). His scientific work has focused on the actions of various peripheral hormones in the central nervous system that serve to regulate food intake, body weight, and the regulation of circulating fuels. In particular, he focuses upon the numerous hypothalamic and gastrointestinal peptides and their associated receptors that influence both energy intake as well as peripheral metabolic processes with the aim of developing new treatment strategies for both obesity and diabetes.
Lee M. Kaplan, MD, PhD
Lee M. Kaplan, MD, PhD, is Director of the Obesity, Metabolism & Nutrition Institute at Massachusetts General Hospital (MGH) and Associate Professor of Medicine at Harvard Medical School. He is the Director of the subspecialty Fellowship Program in Obesity Medicine and Nutrition at MGH; Associate Director of the NIH-sponsored Boston-area Obesity and Nutrition Research Center; a member of the NIH Clinical Obesity Research Panel; and past chairman of the Board of the Campaign to End Obesity. Dr. Kaplan’s clinical expertise is in the areas of obesity medicine, gastroenterology, and liver disease. His research program is focused on understanding the mechanisms by which the gastrointestinal tract regulates metabolic function and using physiological and genetic approaches to identify therapeutically relevant subtypes of obesity and its complications.
—-
Introduction
The epidemic of obesity and its associated comorbid conditions impose an increasingly large burden on society—from the individuals affected to the healthcare systems that provide treatment and the employers, governments, and others who underwrite the associated economic costs. There is an urgent need for better treatments of these problems; however, the development and implementation of solutions has been hindered by the complexity and ubiquity of the problem and the widely held perception that obesity is simply a problem of free choice and self control rather than being a disease in the classic, pathophysiological sense. Lifestyle modification has been viewed as the best solution for this problem. Indeed, lifestyle change provides the most common path to durable control of obesity and its complications. Unfortunately, however, its overall efficacy in patients with established obesity, especially moderate-severe obesity, is low (in the range of 1–5% substantial, long-term efficacy).[1]
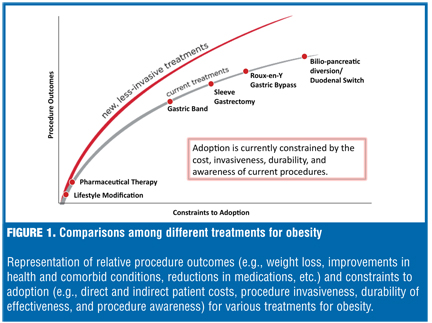
There is strong evidence supporting bariatric surgery as an effective treatment for patients with moderate-to-severe obesity. Recently published data from the Swedish Obesity Subjects Study that included vertical banded gastroplasty, adjustable gastric banding, and Roux-en-Y gastric bypass (RYGB) demonstrated an average 18 percent total weight loss 20 years after surgery.[2] In this study, RYGB, the current standard of bariatric procedures, was associated with an average 25 percent total weight loss at 20 years.[2] These data are in stark contrast to the results reported for patients obtaining nonsurgical obesity treatments at the same centers, who exhibited an average one percent total weight loss at 20 years.2 Despite the impressive weight loss after bariatric surgery and the associated improvements in mortality and numerous other measures of health,[2–9] adoption of bariatric surgery remains low. Reasons for its limited utilization among surgically eligible patients vary, but likely include the invasiveness (anatomical manipulation, tissue removal, presence of an implant), patients’ lack of knowledge about its efficacy and the durability of the benefits, the associated direct and indirect costs to the patient, and an overall lack of awareness of the available options. Regardless of the reasons, there clearly is a large unmet need for effective therapies for the many people with obesity who do not currently undergo bariatric surgery (Figure 1).
This article, the last in a series highlighting the Metabolic Applied Research Strategy (MARS) initiative supported by Ethicon Endo-Surgery, summarizes key findings about the mechanisms of action underlying bariatric surgery and discusses how they can guide the development of novel strategies and therapies to address this unmet need. Based on recent studies published in the scientific and medical literature and illuminated in this series, our view of obesity and its associated metabolic disorders has changed from a perceived flaw in behavior or character to an effect of disruption in the complex physiological network regulating energy balance and metabolic function. Operations that influence the function of this complex physiological network, such as RYGB or vertical sleeve gastrectomy (VSG), may be viewed as metabolic surgery defined here as alterations of the gastrointestinal (GI) tract that affect cellular and molecular signaling leading to a physiologic improvement in energy balance, nutrient utilization, and metabolic disorders.
Findings from MARS can be used to influence investments in novel therapy development. The third article in this series refutes the belief that bariatric surgery induces weight loss primarily by mechanical restriction and nutrient malabsorption.10 One key implication of this observation is that new therapies need not preferentially exploit mechanical manipulations of the GI tract with the express goal of inducing mechanical restriction or limiting absorption of ingested nutrients. Therapies targeting physiological mechanisms known to mediate outcomes from procedures like RYGB may have a higher likelihood of success. One such target identified through the MARS initiative is the selective activation of brown adipose tissue (BAT), a key physiological regulator of energy expenditure following RYGB. Stylopoulos et al11 report that increases in energy expenditure may account for up to half of the weight loss associated with RYGB in several preclinical models. Further evidence suggests that RYGB induces significant activity in BAT.[12] Thus, novel methods to chronically and selectively activate BAT through minimally invasive approaches may be an attractive therapy for obesity.
Using a rodent model of ileal interposition (transposition) surgery (IIS), Kohli et al[13] observed profound changes in the serum bile acid profiles in animals receiving IIS compared to sham-operated controls. These changes corresponded with a reversal in several components of the metabolic syndrome in animals without significant changes in body weight. These effects suggest that selective modulation of bile acid signaling through bile diversion or other means may be an attractive and novel approach to the treatment of the metabolic syndrome. An improved understanding of the mechanisms underlying the changes in bile acid signaling following IIS should further guide the development of such therapies.
While the magnitude of the therapeutic benefits from either isolated BAT activation or bile diversion remains unknown, targeted manipulation of these physiological systems may be achieved less invasively and consequently with less risk than with existing surgical procedures. Used alone or as a means of augmenting the efficacy of existing metabolic operations, such novel therapies could substantially widen the population that benefits from therapies that target the GI tract. As an example, adjustable gastric banding, a procedure that has been shown not to increase energy expenditure or alter bile acid signaling, may be an ideal candidate for augmentation by one or both of these approaches.
Insights from the MARS initiative also raise new questions about which patients will respond best to which procedures, not based solely on their psychological, behavioral, or similar profiles, but on their physiological and genetic makeup. The sixth article in this series describes studies that indicate that patient behavior is not the primary determinant of outcomes after bariatric surgery.[14] While clinical measures, including pre-operative body mass index (BMI), type 2 diabetes mellitus (T2DM) history, capacity for physical activity, education level, and participation in postoperative care, are associated with significantly better weight loss after RYGB,[15] they do not provide sufficient discriminatory power to drive clinical decision making. Recent reports suggest a significant genetic contribution to outcomes following RYGB,[16] and studies to identify those genetic factors are ongoing. With an improved understanding of the key factors that influence weight loss and other benefits of bariatric surgery, better prediction of outcomes will be possible, enhancing patient-physician communication and clinical decision-making, and leading to improved matching of patients and procedures.
The path to new therapies for the treatment of obesity and its associated comorbid conditions is filled with significant hurdles, including complex physiology, incomplete understanding, social stigma, and a stringent regulatory environment. Despite the enormous unmet clinical need, these factors have hindered new advancements in therapy. Better insights into the complex pathophysiology of obesity and metabolic disease as well as innovative strategies for developing effective therapies are essential if we are to succeed where others have failed. The MARS initiative is one such approach. By deconstructing the mechanisms of action of metabolic surgical procedures already proven to be effective, we can accelerate the development of novel therapies to help this large and underserved population. Through MARS and similar efforts supported by various health institutes and corporations around the world, new tools will be developed to improve understanding and education, enhance outcomes for existing therapies, and provide fresh solutions to this global and burgeoning problem.
References
1. Bray GA. Lifestyle and pharmacological approaches to weight loss: efficacy and safety. J Clin Endocrinol Metab. 2008; 93(11 Suppl 1): S81–S88.
2. Sjöström L, Peltonen M, Jacobson, P, et al. Bariatric surgery and long-term cardiovascular events. N Engl J Med. 2012; 307(1):56–65.
3. Sjöström L, Lindroos AK, Peltonen M, et al; Swedish Obese Subjects Study Scientific Group. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N Engl J Med. 2004; 351(26):2683–2693.
4. Karlsson J, Taft C, Rydén A, et al. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes (Lond). 2007;31(8):1248–1261.
5. Sjöström L, Gummesson A, Sjöström CD, et al. Effects of bariatric surgery on cancer incidence in obese patients in Sweden (Swedish Obese Subjects Study): a prospective, controlled intervention trial. Lancet Oncol. 2009;10(7):653–662.
6. Schauer PR, Kashyap SR, Wolski K, et al. Bariatric surgery versus intensive medical therapy in obese patients with diabetes. N Engl J Med. 2012;366(17):1567–1576.
7. Mingrone G, Panunzi S, De Gaetano A, et al. Bariatric surgery versus conventional medical therapy for type 2 diabetes. N Engl J Med. 2012; 366(17):1577–1585.
8. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic review and meta-analysis. JAMA. 2004; 292(14):1724–1737.
9. Sjöström L, Narbro K, Sjöström CD, et al; Swedish Obese Subjects Study. Effects of bariatric surgery on mortality in Swedish obese subjects. N Engl J Med. 2007; 357(8):741–752.
10. Kaplan LM, Seeley RJ, Harris JL. Myths associated with obesity and bariatric surgery. Myth 2: Bariatric surgery induces weight loss primarily by mechanical restriction and nutrient malabsorption. Bariatric Times. 2012; 9(5):12–13.
11. Stylopoulos N, Hoppin AG, Kaplan LM. Roux-en-Y gastric bypass enhances energy expenditure and extends lifespan in diet-induced obese rats. Obesity. 2009;17:1839–1847.
12. Stylopoulos N, Zhang XB, Brownell AL, Kaplan LM. Roux-en-Y Gastric bypass activates brown adipose tssue and increases energy expenditure in obese mice. Gastroenterology. 2012; 138(5 Supplement 1):S-754.
13. Kohli R, Kirby M, Setchell KD, et al. Intestinal adaptation after ileal interposition surgery increases bile acid recycling and protects against obesity-related comorbidities. Am J Physiol Gastrointest Liver Physiol. 2010;299(3):G652–G660. Epub 2010 Jul 1.
14. Kaplan LM, Seeley RJ, Harris JL. Myths associated with obesity and bariatric surgery. Myth 5: Patient behavior is the primary determinant of outcomes after bariatric surgery. Bariatric Times. 2012; 9(8):8–10.
15. Hatoum IJ, Stein HK, Merrifield BF, Kaplan LM. Capacity for physical activity predicts weight loss after Roux-en-Y gastric bypass. Obesity. 2009; 17(1):92–99.
16. Hatoum IJ, Greenawalt DM, Cotsapas C, et al. Heritability of the weight loss response to gastric bypass surgery. J Clin Endocrinol Metab. 2011; 96(10):E1630–E1633.
Category: MARS Initiative Series, Past Articles
Subscribe
If you enjoyed this article, subscribe to receive more just like it.



{kind=link}